

Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: a systematic review and meta-analysis
- PMID: 28245858
- PMCID: PMC5331643
- DOI: 10.1186/s13643-017-0435-5
Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: a systematic review and meta-analysis
Abstract
Background: Stroke can lead to significant impairment of upper limb function which affects performance of activities of daily living (ADL). Functional electrical stimulation (FES) involves electrical stimulation of motor neurons such that muscle groups contract and create or augment a moment about a joint. Whilst lower limb FES was established in post-stroke rehabilitation, there is a lack of clarity on the effectiveness of upper limb FES. This systematic review aims to evaluate the effectiveness of post-stroke upper limb FES on ADL and motor outcomes.
Methods: Systematic review of randomised controlled trials from MEDLINE, PsychINFO, EMBASE, CENTRAL, ISRCTN, ICTRP and ClinicalTrials.gov. Citation checking of included studies and systematic reviews. Eligibility criteria: participants > 18 years with haemorrhagic/ischaemic stroke, intervention group received upper limb FES plus standard care, control group received standard care. Outcomes were ADL (primary), functional motor ability (secondary) and other motor outcomes (tertiary). Quality assessment using GRADE (Grading of Recommendations Assessment, Development and Evaluation) criteria.
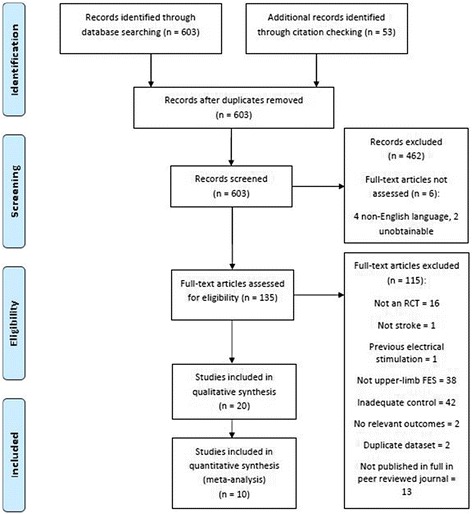
Results: Twenty studies were included. No significant benefit of FES was found for objective ADL measures reported in six studies (standardised mean difference (SMD) 0.64; 95% Confidence Interval (CI) [-0.02, 1.30]; total participants in FES group (n) = 67); combination of all ADL measures was not possible. Analysis of three studies where FES was initiated on average within 2 months post-stroke showed a significant benefit of FES on ADL (SMD 1.24; CI [0.46, 2.03]; n = 32). In three studies where FES was initiated more than 1 year after stroke, no significant ADL improvements were seen (SMD -0.10; CI [-0.59, 0.38], n = 35). Quality assessment using GRADE found very low quality evidence in all analyses due to heterogeneity, low participant numbers and lack of blinding.
Conclusions: FES is a promising therapy which could play a part in future stroke rehabilitation. This review found a statistically significant benefit from FES applied within 2 months of stroke on the primary outcome of ADL. However, due to the very low (GRADE) quality evidence of these analyses, firm conclusions cannot be drawn about the effectiveness of FES or its optimum therapeutic window. Hence, there is a need for high quality large-scale randomised controlled trials of upper limb FES after stroke.
Trial registration: PROSPERO: CRD42015025162 , Date:11/08/2015.
Keywords: Functional electrical stimulation; Meta-analysis, neurorehabilitation; Stroke; Systematic review; Upper limb.
Figures
References
-
- Lynch CL, Popovic MR. Functional electrical stimulation. IEEE Control Syst Mag. 2008;28(2):40–50. doi: 10.1109/MCS.2007.914692. - DOI
-
- Franceschini M, La Porta F, Agosti M, et al. Is health-related-quality of life of stroke patients influenced by neurological impairments at one year after stroke? Eur J Phys Rehabil Med. 2010;46(3):389–399. - PubMed
Included Studies:
-
- A1. Barker RN, Brauer S, Carson R. Training-induced changes in the pattern of triceps to biceps activation during reaching tasks after chronic and severe stroke. Exp Brain Res 2009;196(4):483–96. - PubMed
-
- A2. Cauraugh J, Light K, Kim S, et al. Chronic motor dysfunction after stroke: Recovering wrist and finger extension by electromyography-triggered neuromuscular stimulation. Stroke 2000;31(6):1360–64. - PubMed
-
- A3. Cauraugh JH, Kim S. Two coupled motor recovery protocols are better than one: Electromyogram-triggered neuromuscular stimulation and bilateral movements. Stroke 2002;33(6):1589–94. - PubMed
-
- A4. Cauraugh JH, Kim SB. Chronic stroke motor recovery: duration of active neuromuscular stimulation. J Neurol Sci 2003;215(1-2):13–19. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
