

Presence of an interferon signature in individuals who are anti-nuclear antibody positive lacking a systemic autoimmune rheumatic disease diagnosis
- PMID: 28245862
- PMCID: PMC5331647
- DOI: 10.1186/s13075-017-1243-y
Presence of an interferon signature in individuals who are anti-nuclear antibody positive lacking a systemic autoimmune rheumatic disease diagnosis
Abstract
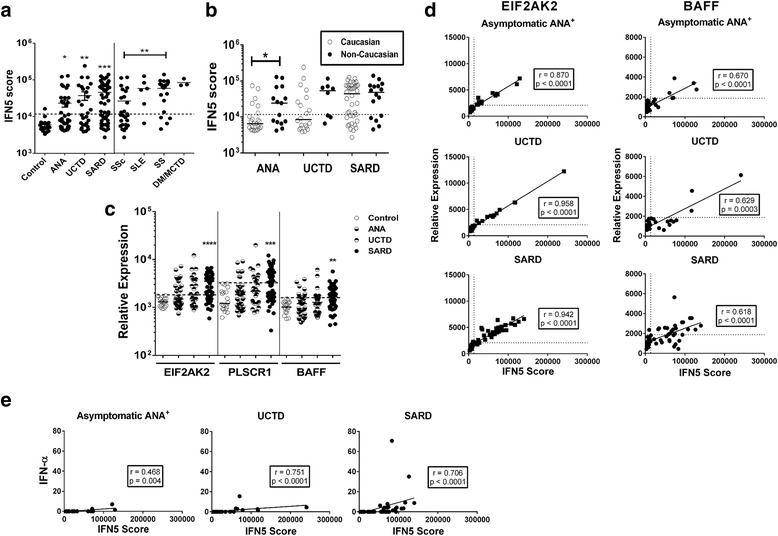
Background: Elevated levels of type I interferons (IFNs) are a characteristic feature of the systemic autoimmune rheumatic diseases (SARDs) and are thought to play an important pathogenic role. However, it is unknown whether these elevations are seen in anti-nuclear antibody-positive (ANA+) individuals who lack sufficient criteria for a SARD diagnosis. We examined IFN-induced gene expression in asymptomatic ANA+ individuals and patients with undifferentiated connective tissue disease (UCTD) to address this question.
Methods: Healthy ANA- control subjects and ANA+ titre (≥1:160 by immunofluorescence) participants meeting no criteria, meeting at least one criterion (UCTD) or meeting SARD classification criteria were recruited. Whole peripheral blood IFN-induced and BAFF gene expression were quantified using NanoString technology. The normalized levels of five IFN-induced genes were summed to produce an IFN5 score.
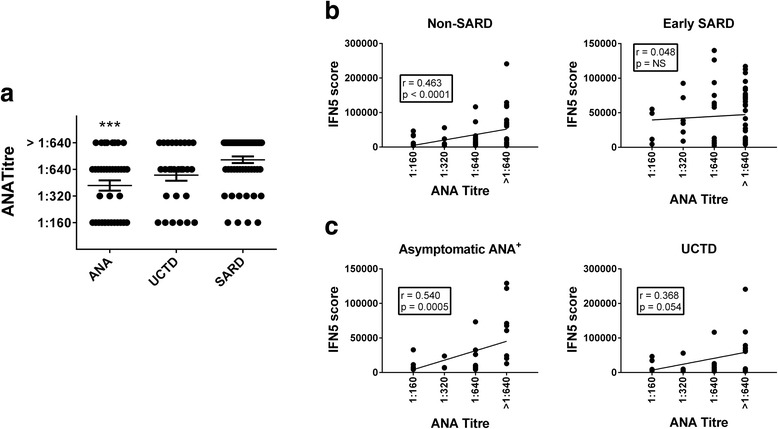
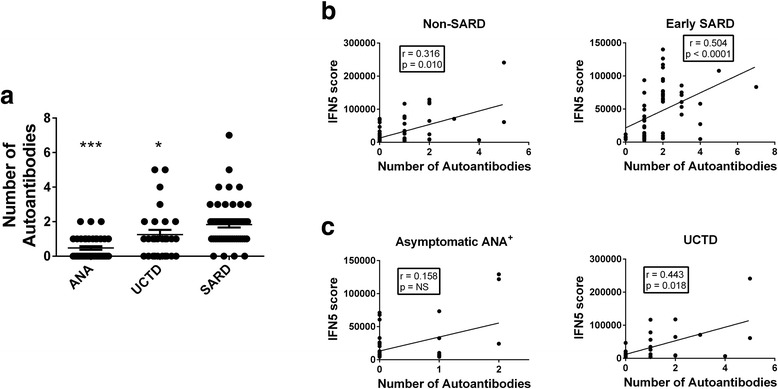
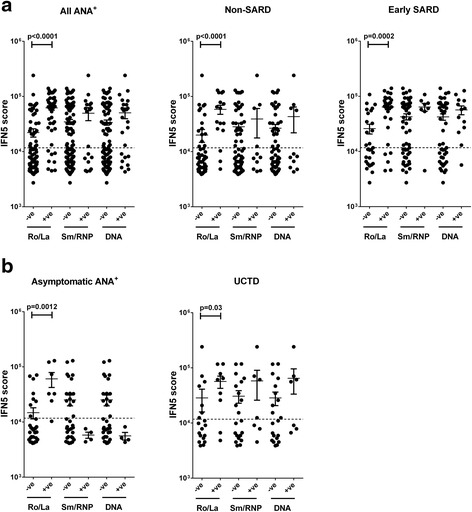
Results: The mean IFN5 scores were increased in all ANA+ participant subsets as compared with healthy control subjects. We found that 36.8% of asymptomatic ANA+ and 50% of UCTD participants had IFN5 scores >2 SD above the mean for healthy control subjects. In all ANA+ subsets, the IFN5 score correlated with the presence of anti-Ro/La antibodies. In the asymptomatic ANA+ subset, this score also correlated with the ANA titre, whereas in the other ANA+ subsets, it correlated with the number of different ANA specificities. Development of new SARD criteria was seen in individuals with normal and high IFN5 scores.
Conclusions: An IFN signature is seen in a significant proportion of ANA+ individuals and appears to be associated with ANA titre and type of autoantibodies, rather than with the presence or development of clinical SARD symptoms.
Keywords: Anti-nuclear antibodies; Interferon; Pre-clinical; Systemic autoimmune rheumatic disease.
Figures
Similar articles
-
The presence of anti-nuclear antibodies alone is associated with changes in B cell activation and T follicular helper cells similar to those in systemic autoimmune rheumatic disease.Arthritis Res Ther. 2018 Nov 29;20(1):264. doi: 10.1186/s13075-018-1752-3. Arthritis Res Ther. 2018. PMID: 30486869 Free PMC article.
-
Fatigue severity in anti-nuclear antibody-positive individuals does not correlate with pro-inflammatory cytokine levels or predict imminent progression to symptomatic disease.Arthritis Res Ther. 2019 Nov 4;21(1):223. doi: 10.1186/s13075-019-2013-9. Arthritis Res Ther. 2019. PMID: 31685018 Free PMC article.
-
Autoantibodies Against DFS70/LEDGF Exclusion Markers for Systemic Autoimmune Rheumatic Diseases (SARD).Clin Lab. 2016;62(4):499-517. doi: 10.7754/clin.lab.2015.150905. Clin Lab. 2016. PMID: 27215068 Review.
-
Interferon and interferon-induced cytokines as markers of impending clinical progression in ANA+ individuals without a systemic autoimmune rheumatic disease diagnosis.Arthritis Res Ther. 2023 Feb 10;25(1):21. doi: 10.1186/s13075-023-02997-w. Arthritis Res Ther. 2023. PMID: 36765391 Free PMC article.
-
Importance of the dense fine speckled pattern on HEp-2 cells and anti-DFS70 antibodies for the diagnosis of systemic autoimmune diseases.Autoimmun Rev. 2012 Jul;11(9):642-5. doi: 10.1016/j.autrev.2011.11.005. Epub 2011 Nov 11. Autoimmun Rev. 2012. PMID: 22100330 Review.
Cited by
-
Differentiating central nervous system demyelinating disorders: The role of clinical, laboratory, imaging characteristics and peripheral blood type I interferon activity.Front Pharmacol. 2022 Aug 12;13:898049. doi: 10.3389/fphar.2022.898049. eCollection 2022. Front Pharmacol. 2022. PMID: 36034800 Free PMC article.
-
Optimal Selection of IFN-α-Inducible Genes to Determine Type I Interferon Signature Improves the Diagnosis of Systemic Lupus Erythematosus.Biomedicines. 2023 Mar 12;11(3):864. doi: 10.3390/biomedicines11030864. Biomedicines. 2023. PMID: 36979843 Free PMC article. Review.
-
Type I interferon pathway assays in studies of rheumatic and musculoskeletal diseases: a systematic literature review informing EULAR points to consider.RMD Open. 2023 Mar;9(1):e002876. doi: 10.1136/rmdopen-2022-002876. RMD Open. 2023. PMID: 36863752 Free PMC article.
-
Shared and unique immune alterations in pre-clinical autoimmunity.Curr Opin Immunol. 2019 Dec;61:60-68. doi: 10.1016/j.coi.2019.08.006. Epub 2019 Sep 23. Curr Opin Immunol. 2019. PMID: 31557691 Free PMC article. Review.
-
Longitudinal Occurrence and Predictors of Patient-Provider Discordance Between Global Assessments of Disease Activity in Rheumatoid Arthritis: A Case-Control Study.Arthritis Care Res (Hoboken). 2020 Jan;72(1):18-26. doi: 10.1002/acr.23819. Epub 2019 Dec 10. Arthritis Care Res (Hoboken). 2020. PMID: 30506552 Free PMC article.
References
-
- Alarcon-Segovia D, Alarcon-Riquelme ME, Cardiel MH, Caeiro F, Massardo L, Villa AR, et al. Familial aggregation of systemic lupus erythematosus, rheumatoid arthritis, and other autoimmune diseases in 1,177 lupus patients from the GLADEL cohort. Arthritis Rheum. 2005;52:1138–47. doi: 10.1002/art.20999. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
