

Adiposity and cancer at major anatomical sites: umbrella review of the literature
- PMID: 28246088
- PMCID: PMC5421437
- DOI: 10.1136/bmj.j477
Adiposity and cancer at major anatomical sites: umbrella review of the literature
Abstract
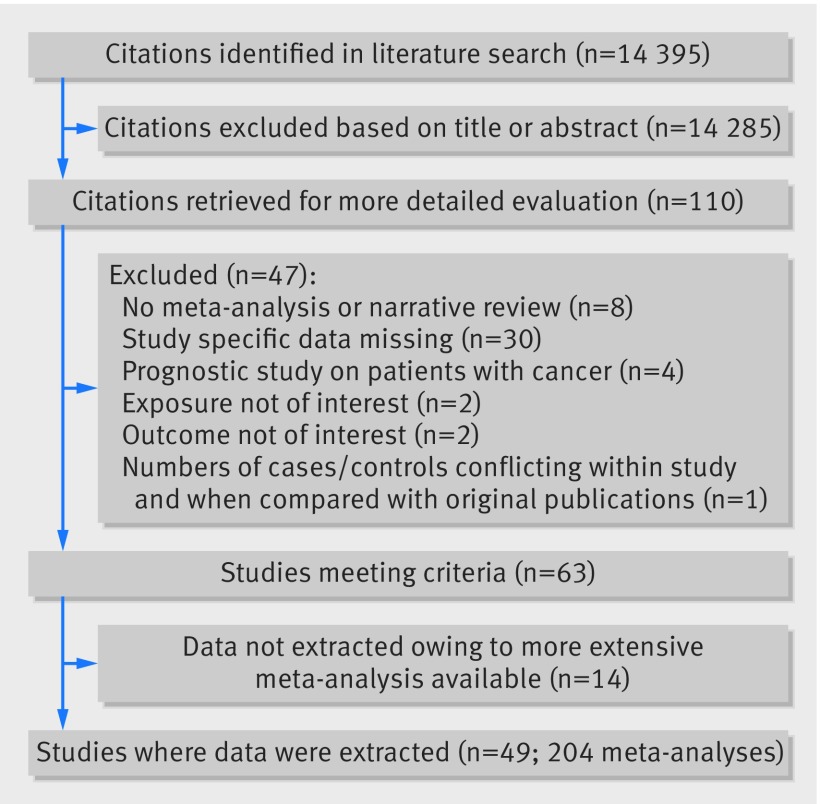
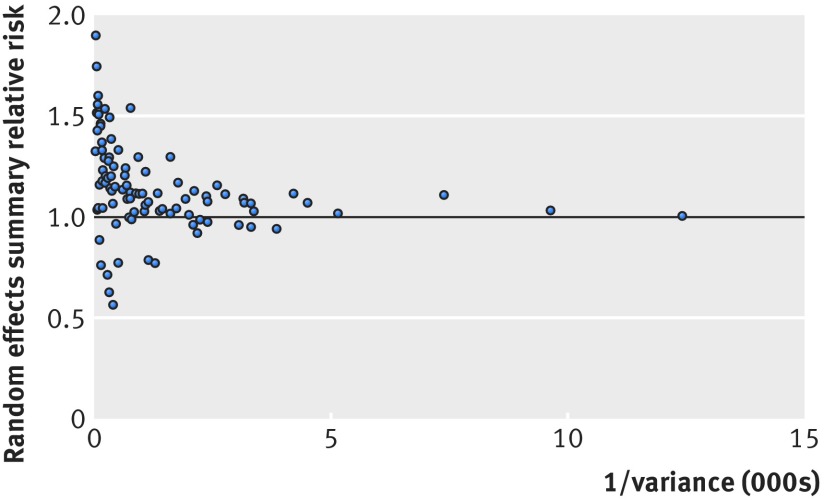
Objective To evaluate the strength and validity of the evidence for the association between adiposity and risk of developing or dying from cancer.Design Umbrella review of systematic reviews and meta-analyses.Data sources PubMed, Embase, Cochrane Database of Systematic Reviews, and manual screening of retrieved references.Eligibility criteria Systematic reviews or meta-analyses of observational studies that evaluated the association between indices of adiposity and risk of developing or dying from cancer.Data synthesis Primary analysis focused on cohort studies exploring associations for continuous measures of adiposity. The evidence was graded into strong, highly suggestive, suggestive, or weak after applying criteria that included the statistical significance of the random effects summary estimate and of the largest study in a meta-analysis, the number of cancer cases, heterogeneity between studies, 95% prediction intervals, small study effects, excess significance bias, and sensitivity analysis with credibility ceilings.Results 204 meta-analyses investigated associations between seven indices of adiposity and developing or dying from 36 primary cancers and their subtypes. Of the 95 meta-analyses that included cohort studies and used a continuous scale to measure adiposity, only 12 (13%) associations for nine cancers were supported by strong evidence. An increase in body mass index was associated with a higher risk of developing oesophageal adenocarcinoma; colon and rectal cancer in men; biliary tract system and pancreatic cancer; endometrial cancer in premenopausal women; kidney cancer; and multiple myeloma. Weight gain and waist to hip circumference ratio were associated with higher risks of postmenopausal breast cancer in women who have never used hormone replacement therapy and endometrial cancer, respectively. The increase in the risk of developing cancer for every 5 kg/m2 increase in body mass index ranged from 9% (relative risk 1.09, 95% confidence interval 1.06 to 1.13) for rectal cancer among men to 56% (1.56, 1.34 to 1.81) for biliary tract system cancer. The risk of postmenopausal breast cancer among women who have never used HRT increased by 11% for each 5 kg of weight gain in adulthood (1.11, 1.09 to 1.13), and the risk of endometrial cancer increased by 21% for each 0.1 increase in waist to hip ratio (1.21, 1.13 to 1.29). Five additional associations were supported by strong evidence when categorical measures of adiposity were included: weight gain with colorectal cancer; body mass index with gallbladder, gastric cardia, and ovarian cancer; and multiple myeloma mortality.Conclusions Although the association of adiposity with cancer risk has been extensively studied, associations for only 11 cancers (oesophageal adenocarcinoma, multiple myeloma, and cancers of the gastric cardia, colon, rectum, biliary tract system, pancreas, breast, endometrium, ovary, and kidney) were supported by strong evidence. Other associations could be genuine, but substantial uncertainty remains. Obesity is becoming one of the biggest problems in public health; evidence on the strength of the associated risks may allow finer selection of those at higher risk of cancer, who could be targeted for personalised prevention strategies.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Fresh evidence links adiposity with multiple cancers.BMJ. 2017 Feb 28;356:j908. doi: 10.1136/bmj.j908. BMJ. 2017. PMID: 28246087 No abstract available.
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-917. 10.1002/ijc.25516 pmid:21351269. - DOI - PubMed
-
- Dixon JB. The effect of obesity on health outcomes. Mol Cell Endocrinol 2010;316:104-8. 10.1016/j.mce.2009.07.008 pmid:19628019. - DOI - PubMed
-
- Stevens GA, Singh GM, Lu Y, et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index). National, regional, and global trends in adult overweight and obesity prevalences. Popul Health Metr 2012;10:22 10.1186/1478-7954-10-22 pmid:23167948. - DOI - PMC - PubMed
-
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016;387:1377-96. 10.1016/S0140-6736(16)30054-X pmid:27115820. - DOI - PMC - PubMed
-
- Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014;384:766-81. 10.1016/S0140-6736(14)60460-8 pmid:24880830. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical