

Cystic adrenal lesions: focus on pediatric population (a review)
- PMID: 28246490
- PMCID: PMC5305088
- DOI: 10.15386/cjmed-677
Cystic adrenal lesions: focus on pediatric population (a review)
Abstract
Background and aim: The cysts may potentially affect any organ; adrenals cysts are rare. This is a review of the literature regarding adrenal cysts, focusing on children and young adults.
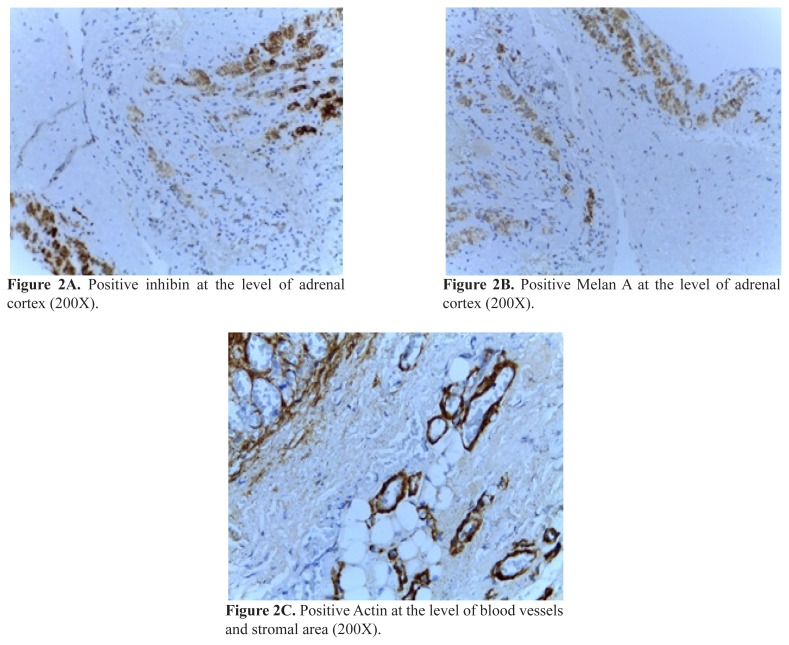
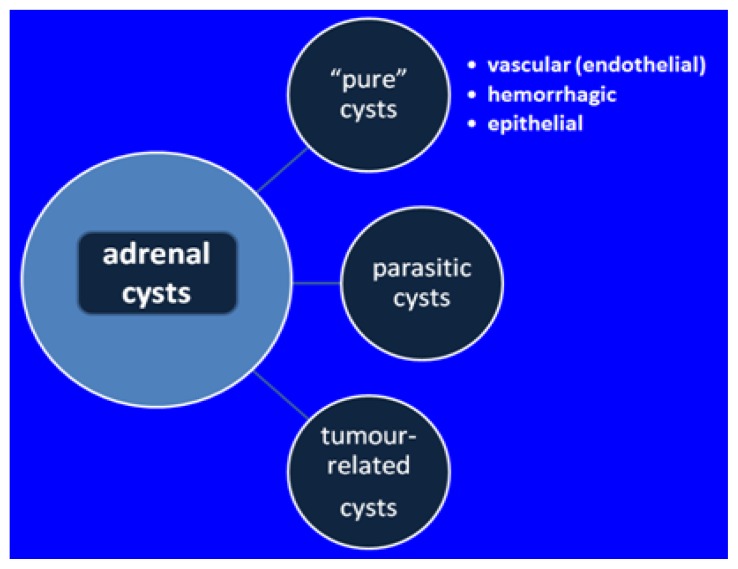
General data: Three major types have been described: pure cysts (endothelial, epithelial, and hemorrhagic or pseudocyst), parasitic (as hydatid) cysts and cystic part of a tumour (most frequent are neuroblastoma, ganglioneuroma, pheocromocytoma, and teratoma). The complications are: bleeding, local pressure effects; infection; rupture (including post-traumatic); arterial hypertension due to renal vessels compression. Adrenal hemorrhage represents a particular condition associating precipitating factors such as: coagulation defects as Factor IX or X deficiency, von Willebrand disease, thrombocytopenia; antiphospholipid syndrome; previous therapy with clopidogrel or corticosteroids; the rupture of a prior tumour. At birth, the most suggestive features are abdominal palpable mass, anemia, and persistent jaundice. Adrenal insufficiency may be found especially in premature delivery. The hemorrhage is mostly self-limiting. Antenatal ultrasound diagnosis of a cyst does not always predict the exact pathology result. The most important differential diagnosis of adrenal hemorrhage/hemorrhagic cyst is cystic neuroblastoma which is highly suggestive in the presence of distant metastases and abnormal catecholamine profile. The major clue to differentiate the two conditions is the fact that the tumor is stable or increases over time while the adrenal hemorrhage is expected to remit within one to two weeks.
Conclusion: Pediatric adrenal cysts vary from simple cysts with a benign behavior to neoplasia- related lesions displaying severe prognosis as seen in cystic neuroblastoma. A multidisciplinary team is required for their management which is conservative as close follow-up or it makes necessary different surgical procedures in cases with large masses or if a malignancy suspicion is presented. Recently, laparoscopic approach is regarded as a safe procedure by some authors but generally, open surgery is more frequent used compare to adults; in most cases the preservation of normal gland is advisable.
Keywords: adrenal cyst; adrenal hemorrhage; cystic neuroblastoma.
Figures

References
-
- Quinn E, McGee R, Nuccio R, Pappo AS, Nichols KE. Genetic Predisposition to Neonatal Tumors. Curr Pediatr Rev. 2015;11(3):164–178. - PubMed
-
- Baudin E Endocrine Tumor Board of Gustave Roussy. Adrenocortical carcinoma. Endocrinol Metab Clin North Am. 2015;44(2):411–434. - PubMed
-
- Elfiky A. Adrenocortical Carcinoma: A Clinician’s Perspective. Surg Pathol Clin. 2015;8(4):751–754. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources