

No-Touch Radiofrequency Ablation: A Comparison of Switching Bipolar and Switching Monopolar Ablation in Ex Vivo Bovine Liver
- PMID: 28246508
- PMCID: PMC5313516
- DOI: 10.3348/kjr.2017.18.2.279
No-Touch Radiofrequency Ablation: A Comparison of Switching Bipolar and Switching Monopolar Ablation in Ex Vivo Bovine Liver
Abstract
Objective: To evaluate the feasibility, efficiency, and safety of no-touch switching bipolar (SB) and switching monopolar (SM) radiofrequency ablation (RFA) using ex vivo bovine livers.
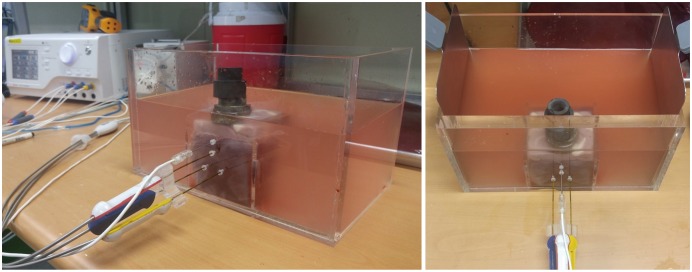
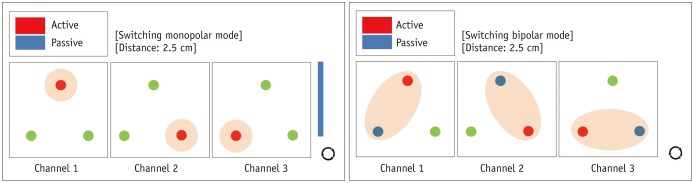
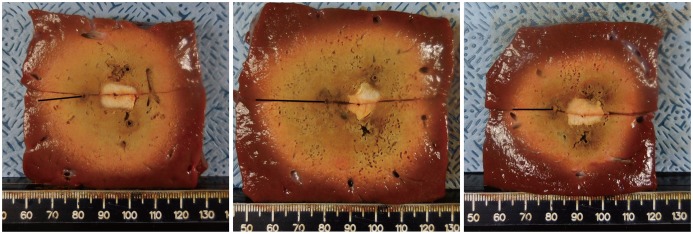
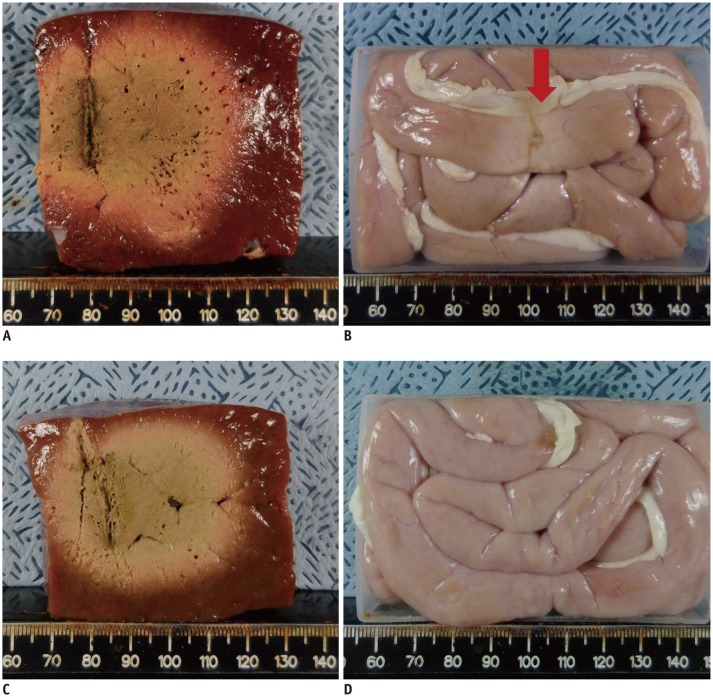
Materials and methods: A pork loin cube was inserted as a tumor mimicker in the bovine liver block; RFA was performed using the no-touch technique in the SM (group A1; 10 minutes, n = 10, group A2; 15 minutes, n = 10) and SB (group B; 10 minutes, n = 10) modes. The groups were compared based on the creation of confluent necrosis with sufficient safety margins, the dimensions, and distance between the electrode and ablation zone margin (DEM). To evaluate safety, small bowel loops were placed above the liver surface and 30 additional ablations were performed in the same groups.
Results: Confluent necroses with sufficient safety margins were created in all specimens. SM RFA created significantly larger volumes of ablation compared to SB RFA (all p < 0.001). The DEM of group B was significantly lower than those of groups A1 and A2 (all p < 0.001). Although thermal injury to the small bowel was noted in 90%, 100%, and 30% of the cases in groups A1, A2, and B, respectively, full depth injury was noted only in 60% of group A2 cases.
Conclusion: The no-touch RFA technique is feasible in both the SB and SM modes; however, SB RFA appears to be more advantageous compared to SM RFA in the creation of an ablation zone while avoiding the unnecessary creation of an adjacent parenchymal ablation zone or adjacent small bowel injuries.
Keywords: Bovine; Hepatocellular carcinoma; Minimally invasive; No-touch technique; Preclinical; Radiofrequency ablation.
Figures
Comment in
-
RE: Should We Use a Monopolar or Bipolar Mode for Performing No-Touch Radiofrequency Ablation of Liver Tumors? Clinical Practice Might have Already Resolved the Matter Once and for All.Korean J Radiol. 2017 Jul-Aug;18(4):749-752. doi: 10.3348/kjr.2017.18.4.749. Epub 2017 May 19. Korean J Radiol. 2017. PMID: 28670170 Free PMC article. No abstract available.
Similar articles
-
No-touch radiofrequency ablation using multiple electrodes: An in vivo comparison study of switching monopolar versus switching bipolar modes in porcine livers.PLoS One. 2017 Apr 26;12(4):e0176350. doi: 10.1371/journal.pone.0176350. eCollection 2017. PLoS One. 2017. PMID: 28445542 Free PMC article.
-
Ex vivo experiment of saline-enhanced hepatic bipolar radiofrequency ablation with a perfused needle electrode: comparison with conventional monopolar and simultaneous monopolar modes.Cardiovasc Intervent Radiol. 2005 May-Jun;28(3):338-45. doi: 10.1007/s00270-004-0177-3. Cardiovasc Intervent Radiol. 2005. PMID: 15789259
-
Switching bipolar hepatic radiofrequency ablation using internally cooled wet electrodes: comparison with consecutive monopolar and switching monopolar modes.Br J Radiol. 2015 Jun;88(1050):20140468. doi: 10.1259/bjr.20140468. Epub 2015 Apr 15. Br J Radiol. 2015. PMID: 25873479 Free PMC article.
-
Saline-Infused Radiofrequency Ablation: A Review on the Key Factors for a Safe and Reliable Tumour Treatment.IEEE Rev Biomed Eng. 2024;17:310-321. doi: 10.1109/RBME.2022.3179742. Epub 2024 Jan 12. IEEE Rev Biomed Eng. 2024. PMID: 35653443 Review.
-
Current opinion: optimize radiofrequency ablation through electrophysiological principles, modeling, and clinical recommendations.Curr Opin Anaesthesiol. 2024 Oct 1;37(5):553-564. doi: 10.1097/ACO.0000000000001419. Epub 2024 Aug 12. Curr Opin Anaesthesiol. 2024. PMID: 39145613 Review.
Cited by
-
RE: Should We Use a Monopolar or Bipolar Mode for Performing No-Touch Radiofrequency Ablation of Liver Tumors? Clinical Practice Might have Already Resolved the Matter Once and for All.Korean J Radiol. 2017 Jul-Aug;18(4):749-752. doi: 10.3348/kjr.2017.18.4.749. Epub 2017 May 19. Korean J Radiol. 2017. PMID: 28670170 Free PMC article. No abstract available.
-
Radiofrequency ablation using internally cooled wet electrodes in bipolar mode for the treatment of recurrent hepatocellular carcinoma after locoregional treatment: A randomized prospective comparative study.PLoS One. 2020 Sep 28;15(9):e0239733. doi: 10.1371/journal.pone.0239733. eCollection 2020. PLoS One. 2020. PMID: 32986758 Free PMC article. Clinical Trial.
-
A Glimpse on Trends and Characteristics of Recent Articles Published in the Korean Journal of Radiology.Korean J Radiol. 2019 Dec;20(12):1555-1561. doi: 10.3348/kjr.2019.0928. Korean J Radiol. 2019. PMID: 31854145 Free PMC article. No abstract available.
-
No-Touch Radiofrequency Ablation of VX2 Hepatic Tumors In Vivo in Rabbits: A Proof of Concept Study.Korean J Radiol. 2018 Nov-Dec;19(6):1099-1109. doi: 10.3348/kjr.2018.19.6.1099. Epub 2018 Oct 18. Korean J Radiol. 2018. PMID: 30386141 Free PMC article.
-
New Biparietal Bipolar Catheter Prototype for Hybrid Atrial Fibrillation Ablation.Innovations (Phila). 2021 Mar-Apr;16(2):181-187. doi: 10.1177/1556984520981025. Epub 2021 Jan 7. Innovations (Phila). 2021. PMID: 33410714 Free PMC article.
References
-
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943. - PubMed
-
- Salhab M, Canelo R. An overview of evidence-based management of hepatocellular carcinoma: a meta-analysis. J Cancer Res Ther. 2011;7:463–475. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
