

Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Salivary Gland
- PMID: 28247227
- PMCID: PMC5340736
- DOI: 10.1007/s12105-017-0795-0
Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Salivary Gland
Abstract
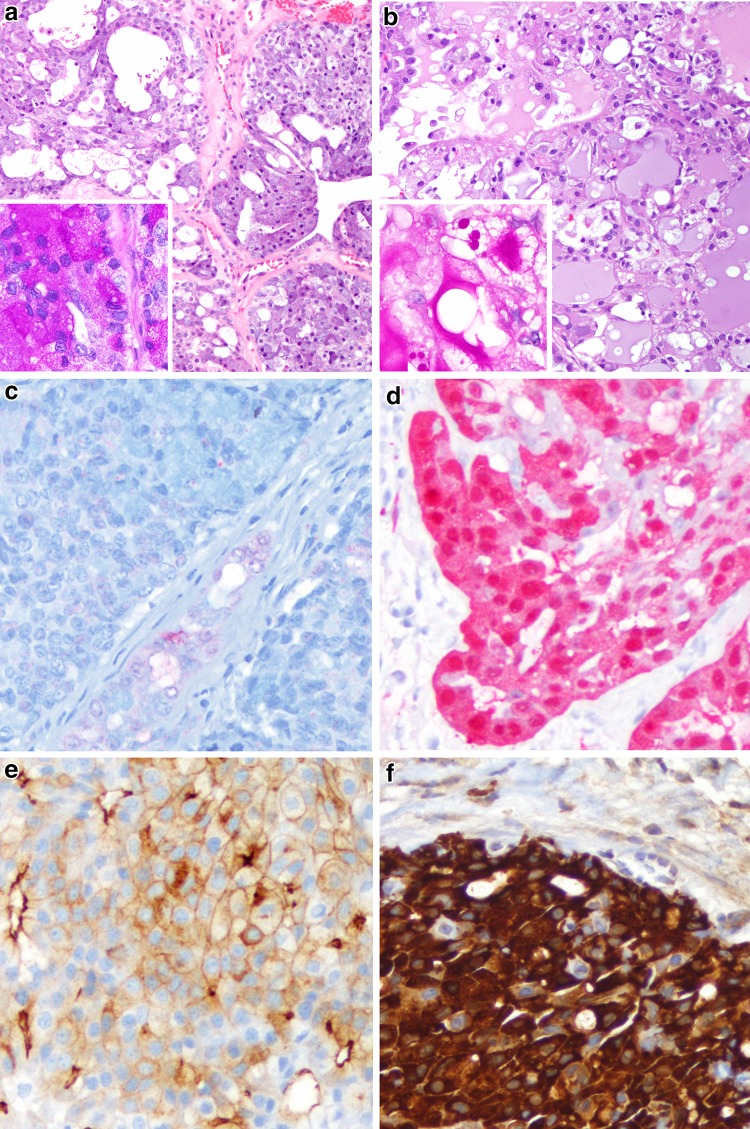
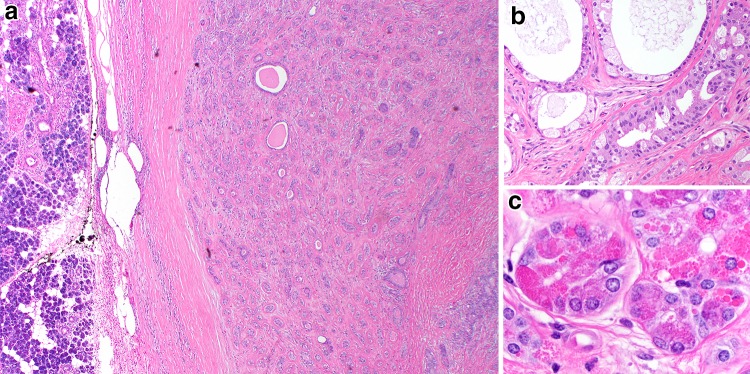
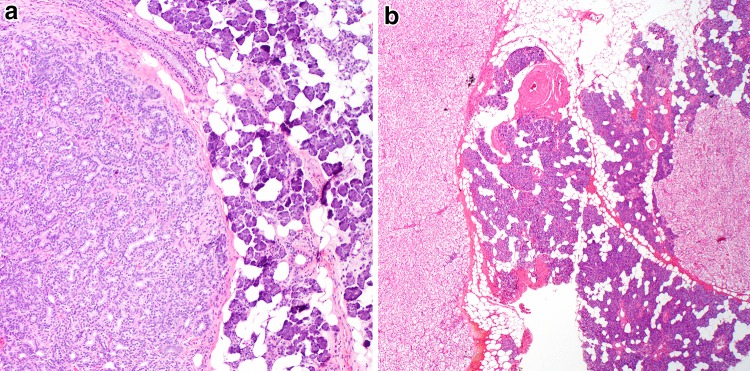
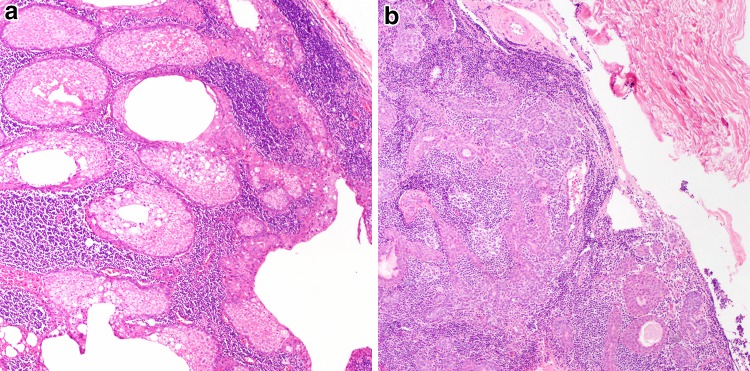
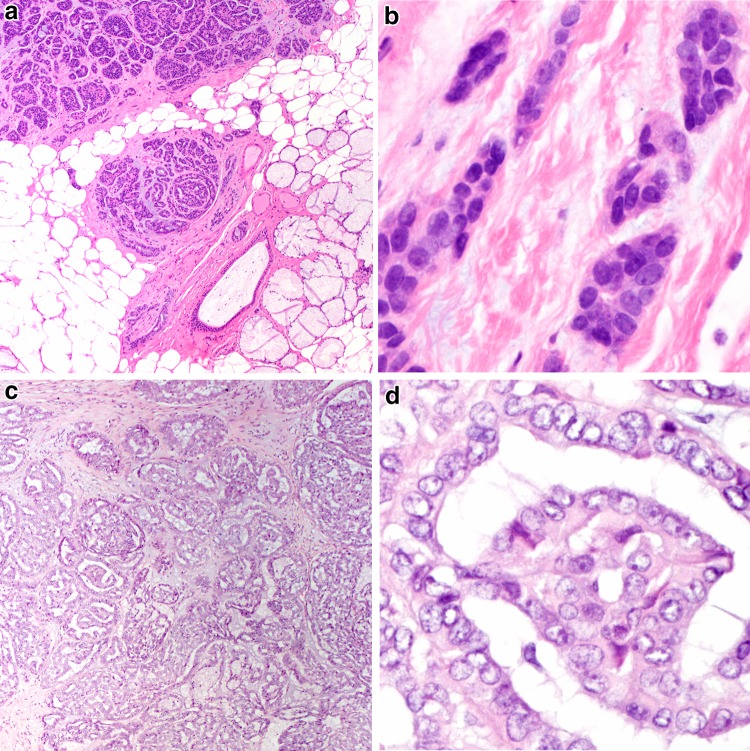
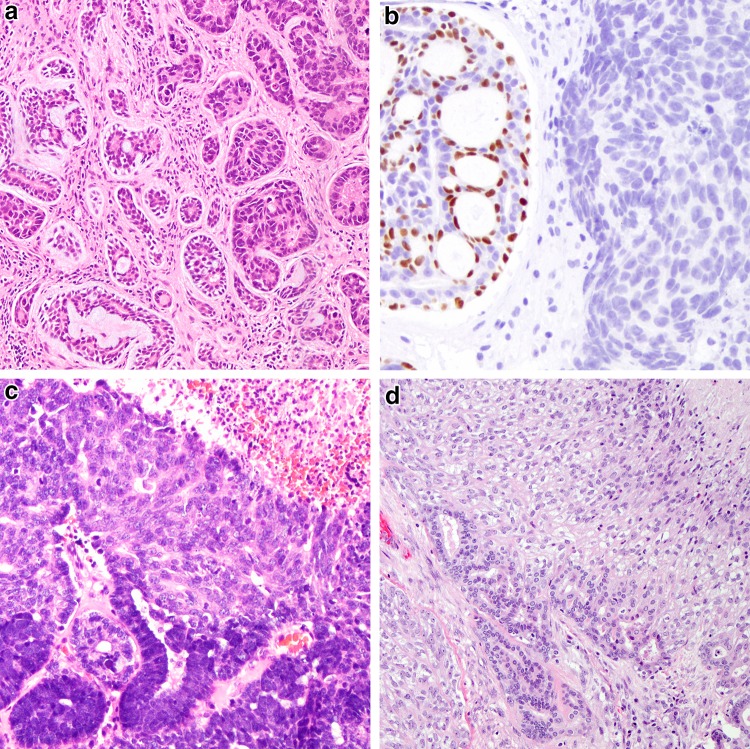
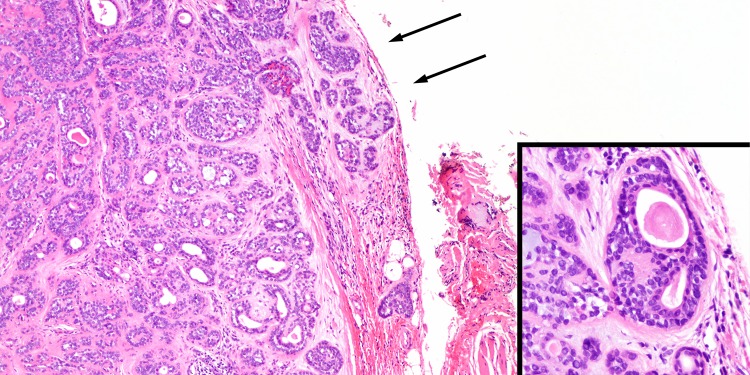
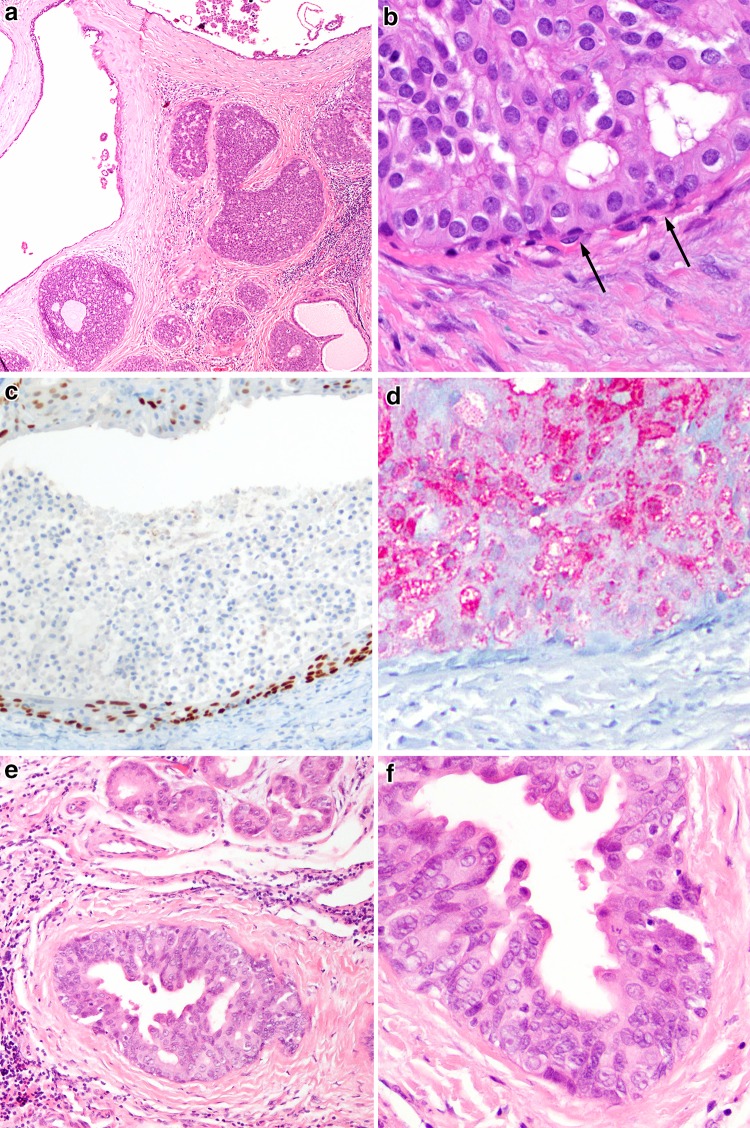
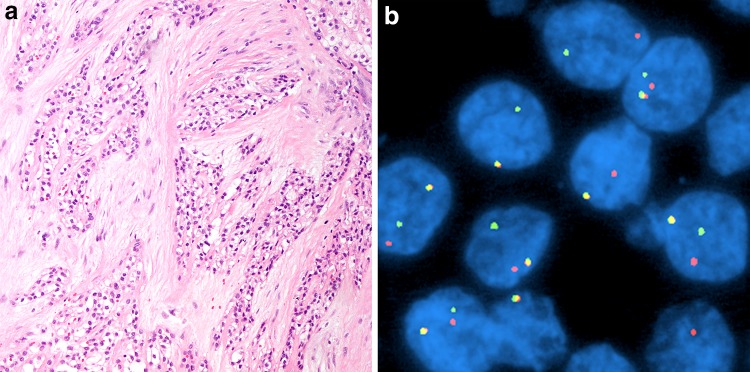
The salivary gland section in the 4th edition of the World Health Organization classification of head and neck tumors features the description and inclusion of several entities, the most significant of which is represented by (mammary analogue) secretory carcinoma. This entity was extracted mainly from acinic cell carcinoma based on recapitulation of breast secretory carcinoma and a shared ETV6-NTRK3 gene fusion. Also new is the subsection of "Other epithelial lesions," for which key entities include sclerosing polycystic adenosis and intercalated duct hyperplasia. Many entities have been compressed into their broader categories given clinical and morphologic similarities, or transitioned to a different grouping as was the case with low-grade cribriform cystadenocarcinoma reclassified as intraductal carcinoma (with the applied qualifier of low-grade). Specific grade has been removed from the names of the salivary gland entities such as polymorphous adenocarcinoma, providing pathologists flexibility in assigning grade and allowing for recognition of a broader spectrum within an entity. Cribriform adenocarcinoma of (minor) salivary gland origin continues to be divisive in terms of whether it should be recognized as a distinct category. This chapter also features new key concepts such as high-grade transformation. The new paradigm of translocations and gene fusions being common in salivary gland tumors is featured heavily in this chapter.
Keywords: Classification; Correlative; Molecular; Neoplasia; Salivary gland; Translocations; World Health Organization.
Conflict of interest statement
Conflict of interest
The authors have no financial or other conflicts of interest to report.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
References
-
- Eveson JW, Auclair PL, Gnepp DR, El-Naggar AK. Tumours of the salivary gland. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization classification of tumours: pathology and genetics of head and neck tumours. Lyon: IARC; 2005. p. 164.
-
- Skalova A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34(5):599–608. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
