

Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Oropharynx
- PMID: 28247229
- PMCID: PMC5340734
- DOI: 10.1007/s12105-017-0793-2
Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Oropharynx
Abstract
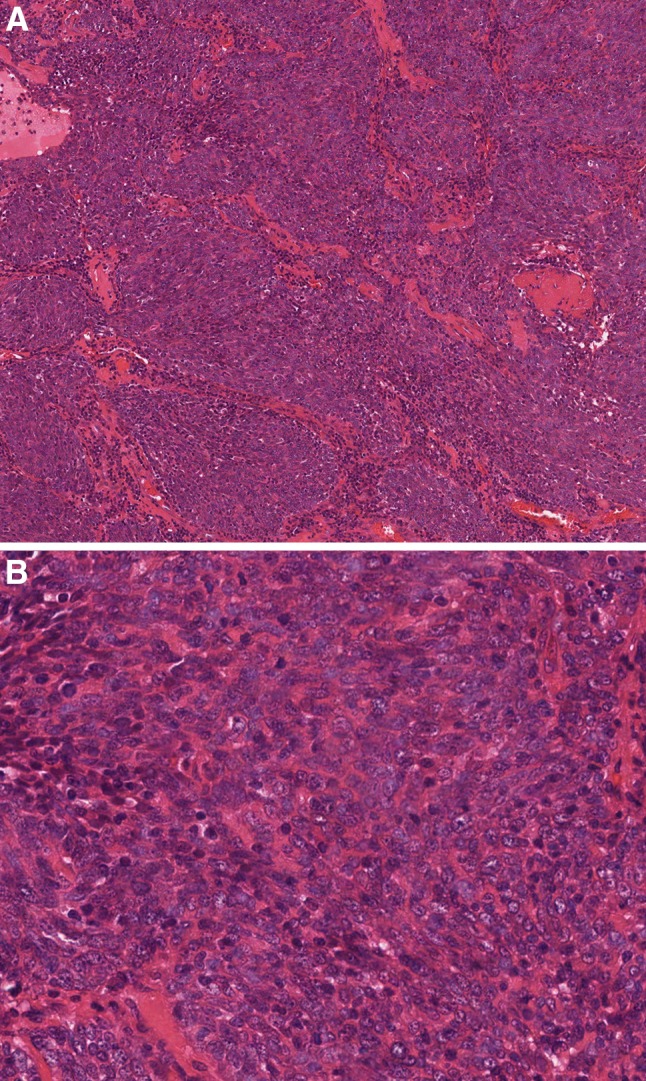
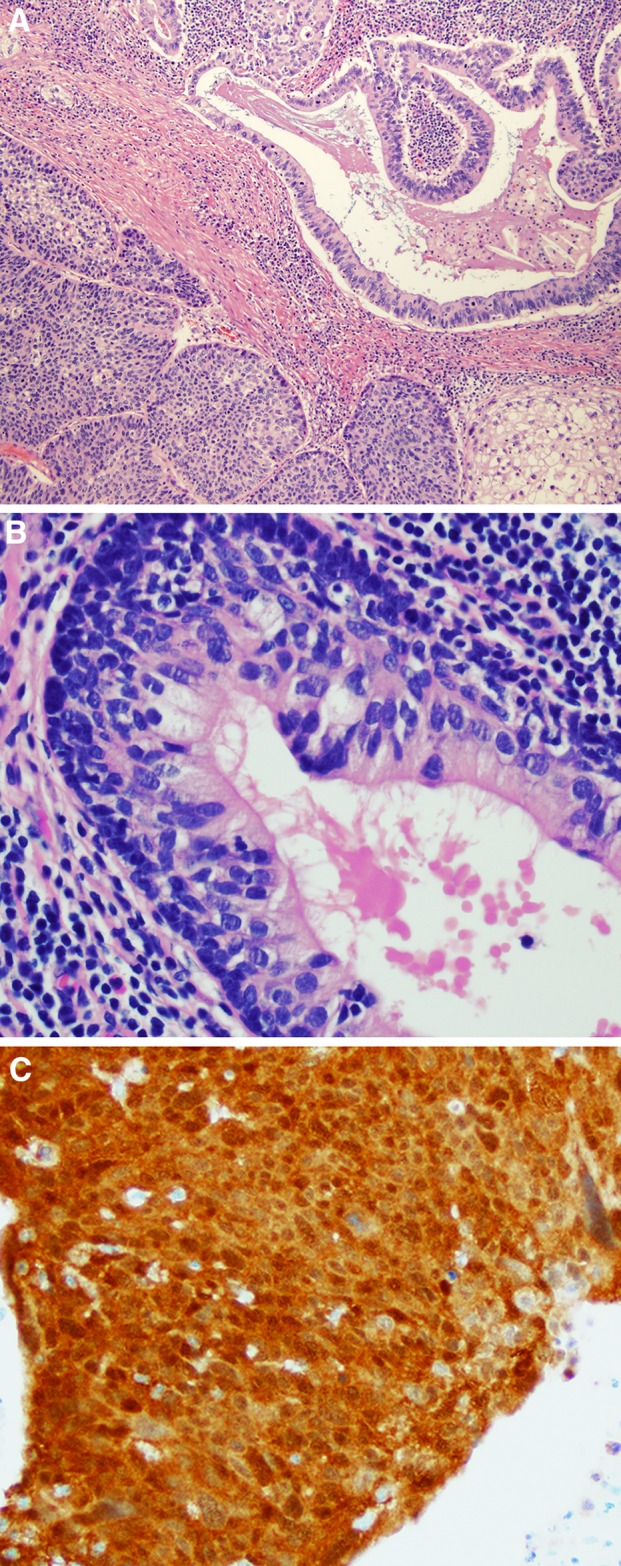
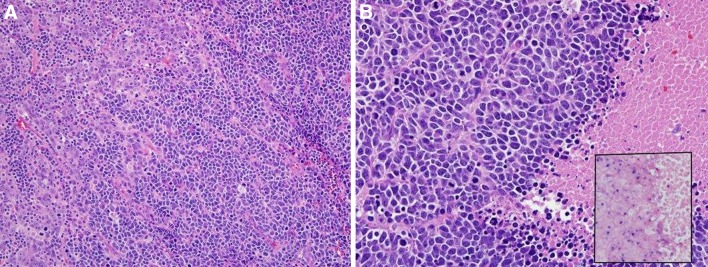
The changes for oropharyngeal lesions in the 2017 edition of the WHO/IARC Classification of Head and Neck Tumours reference book are dramatic and significant, largely due to the growing impact of high risk human papillomavirus (HPV). The upcoming edition divides tumours of the oral cavity and oropharynx into separate chapters, classifies squamous cell carcinomas (SCC) of the oropharynx on the basis of HPV status, abandons the practice of histologic grading for oropharyngeal SCCs that are HPV positive, recognizes small cell carcinoma of the oropharynx, and combines polymorphous low grade adenocarcinoma and cribriform adenocarcinoma of tongue and minor salivary glands under the single term "polymorphous adenocarcinoma." This review not only calls attention to these changes, but describes the rationale driving these changes and highlights their implications for routine clinical practice.
Keywords: Human papillomavirus; Oropharynx; Polymorphous adenocarcinoma; Small cell carcinoma; Squamous cell carcinoma; World Health Organization.
Conflict of interest statement
Conflict of interest
Neither author has any conflicts of interest to disclose.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures


References
-
- Gondim DD, Haynes W, Wang X, Chernock RD, El-Mofty SK, Lewis JS Jr. Histologic typing in oropharyngeal squamous cell carcinoma: A 4-year prospective practice study with p16 and high-risk HPV mRNA testing correlation. Am J Surg Pathol. 2016. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
