

Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: What is New in the 2017 WHO Blue Book for Tumours of the Hypopharynx, Larynx, Trachea and Parapharyngeal Space
- PMID: 28247231
- PMCID: PMC5340729
- DOI: 10.1007/s12105-017-0788-z
Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: What is New in the 2017 WHO Blue Book for Tumours of the Hypopharynx, Larynx, Trachea and Parapharyngeal Space
Abstract
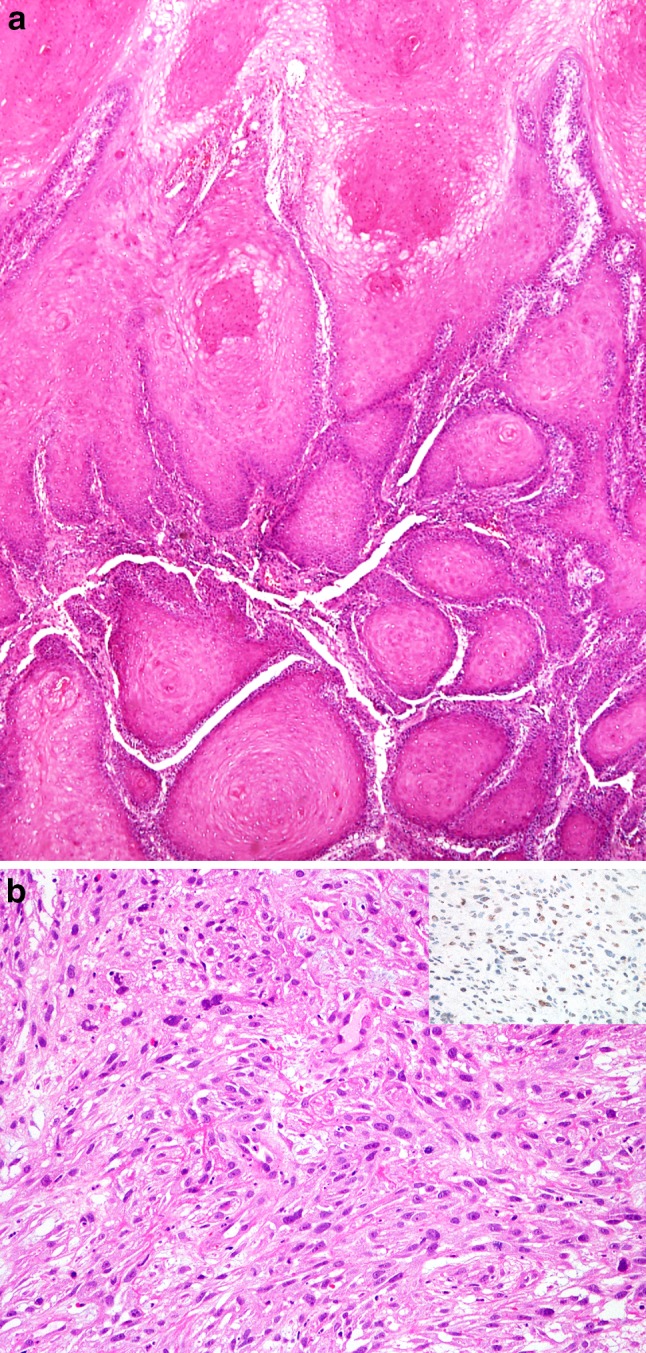
Chapter 3 "Tumours of the hypopharynx, larynx, trachea, and parapharyngeal space" of the World Health Organization (WHO) Blue Book 2017 "Classification of Head and Neck Tumours" shows a shortened list of entities, especially due to reducing the number of benign and malignant soft tissue tumours, malignant melanoma and some others, which are transferred to more frequently affected regions of the head and neck. The basic concept of the new edition is to assimilate all advances concerning the discussed tumours in a shorter framework, appropriate for daily work. The main emphasis is on the most frequent lesions and tumors originating from the covering squamous epithelium. Laryngeal and hypopharyngeal conventional squamous cell carcinoma (CSCC), its variants and precursor lesions, occupy a major part of the chapter. New data on etiopathogenesis, with the focus on human papillomavirus (HPV) infection, are discussed in relation to the entities of the squamous epithelium. Although only a small fraction of these lesions are HPV-related, further studies are required for evaluation of the potential prognostic and therapeutic benefit of mRNA HPV determination. In contrast to earlier data, laryngeal and hypopharyngeal verrucous SCC, spindle cell SCC and basaloid SCC are not anymore considered as HPV-related tumours. New data on the pathogenesis of spindle cell SCC exhibiting divergent differentiation by epithelial-mesenchymal transition, are also briefly discussed. The most important innovation is brought by the section on precursor lesions, in which a unified two-tier classification, consisting of low- and high-grade dysplasia, is introduced. The proposed two-tier system can also be transformed into a three-tier classification for treatment purposes, with a distinction between carcinoma in situ and high-grade dysplasia. The reviewed morphological criteria of the proposed system are based on the amended Ljubljana classification. The section on laryngeal neuroendocrine carcinomas (NEC) represents a considerable improvement in terminology and classification. NEC are divided into well-, moderate- and poorly-differentiated neuroendocrine carcinoma. The latter is additionally divided into small cell NEC and large cell NEC (LCNEC). It is of extreme importance that LCNEC, which was associated in the WHO 2005 edition with atypical carcinoid/moderately differentiated neuroendocrine carcinoma, grade II, has now been transferred into the group of poorly differentiated NEC, grade III, displaying a specific morphology and poorer prognosis.
Keywords: Conventional squamous cell carcinoma; HPV infection; Larynx; Neuroendocrine carcinomas; Precursor lesions, classification; Variants of conventional squamous cell carcinoma.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures



Similar articles
-
Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Hypopharynx, Larynx, Trachea and Parapharyngeal Space.Head Neck Pathol. 2022 Mar;16(1):31-39. doi: 10.1007/s12105-021-01405-6. Epub 2022 Mar 21. Head Neck Pathol. 2022. PMID: 35312977 Free PMC article. Review.
-
Neuroendocrine Carcinomas of the Larynx and Head and Neck: Challenges in Classification and Grading.Head Neck Pathol. 2018 Mar;12(1):1-8. doi: 10.1007/s12105-018-0894-6. Epub 2018 Mar 20. Head Neck Pathol. 2018. PMID: 29557536 Free PMC article.
-
Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: What Is New in the 2017 WHO Blue Book for Tumors and Tumor-Like Lesions of the Neck and Lymph Nodes.Head Neck Pathol. 2017 Mar;11(1):48-54. doi: 10.1007/s12105-017-0796-z. Epub 2017 Feb 28. Head Neck Pathol. 2017. PMID: 28247228 Free PMC article.
-
Recent Changes of Classification for Squamous Intraepithelial Lesions of the Head and Neck.Arch Pathol Lab Med. 2018 Jul;142(7):829-832. doi: 10.5858/arpa.2017-0438-RA. Epub 2018 May 18. Arch Pathol Lab Med. 2018. PMID: 29775074 Review.
-
Large cell neuroendocrine carcinoma of the larynx: definition of an entity.Head Neck Pathol. 2010 Sep;4(3):198-207. doi: 10.1007/s12105-010-0188-0. Epub 2010 Jun 30. Head Neck Pathol. 2010. PMID: 20589486 Free PMC article.
Cited by
-
Vocal fold leukoplakia recurrence risk model.Sci Rep. 2024 Jan 2;14(1):266. doi: 10.1038/s41598-023-50691-3. Sci Rep. 2024. PMID: 38168150 Free PMC article.
-
Combined larynx large cell neuroendocrine and squamous cell carcinoma: a case report.Einstein (Sao Paulo). 2023 Dec 4;21:eRC0618. doi: 10.31744/einstein_journal/2023RC0618. eCollection 2023. Einstein (Sao Paulo). 2023. PMID: 38055554 Free PMC article.
-
Leukoplakia: An Invasive Cancer Hidden within the Vocal Folds. A Multivariate Analysis of Risk Factors.Front Oncol. 2021 Dec 13;11:772255. doi: 10.3389/fonc.2021.772255. eCollection 2021. Front Oncol. 2021. PMID: 34966677 Free PMC article.
-
Serum and tissue expression of neuropilin 1 in precancerous and malignant vocal fold lesions.PLoS One. 2020 Oct 1;15(10):e0239550. doi: 10.1371/journal.pone.0239550. eCollection 2020. PLoS One. 2020. PMID: 33002021 Free PMC article.
-
Rare cases of head and neck's neuroendocrine carcinomas disease: Case series of 4 patients and review of the literature.Int J Surg Case Rep. 2020;66:270-276. doi: 10.1016/j.ijscr.2019.12.003. Epub 2019 Dec 13. Int J Surg Case Rep. 2020. PMID: 31884263 Free PMC article.
References
-
- Fusconi M, Campo F, Gallo A, et al. Laryngeal Cancer, HPV DNA vs E6/E7 mRNA test: a systematic review. J Voice. 2016 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
