

Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Nasal Cavity, Paranasal Sinuses and Skull Base
- PMID: 28247233
- PMCID: PMC5340732
- DOI: 10.1007/s12105-017-0791-4
Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Nasal Cavity, Paranasal Sinuses and Skull Base
Abstract
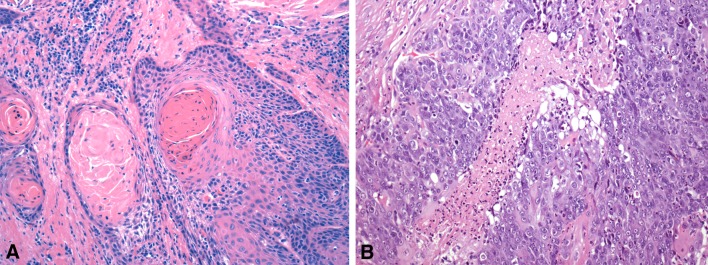
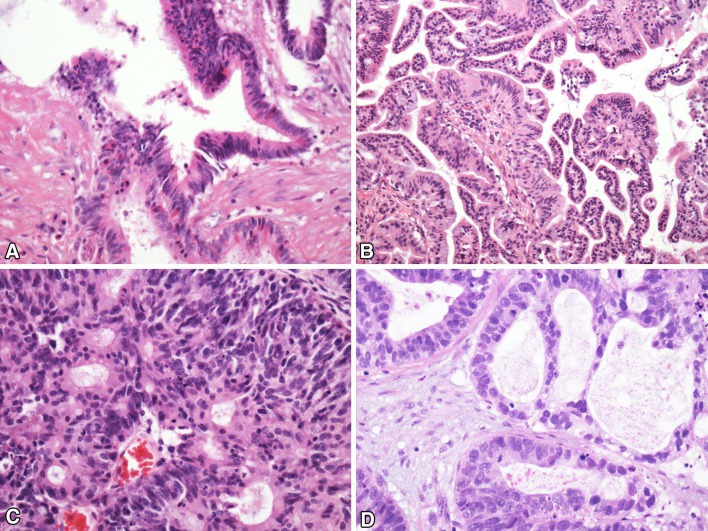
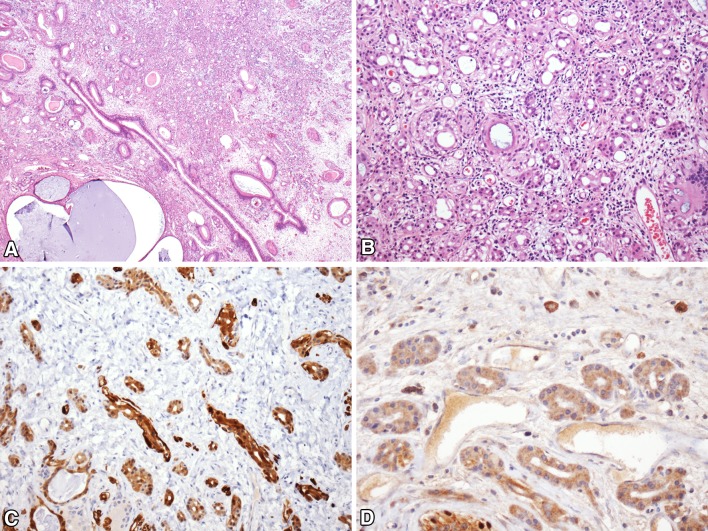
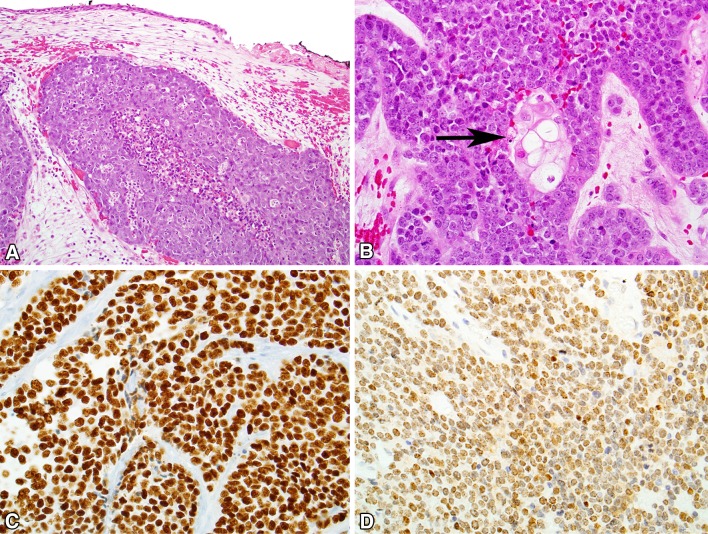
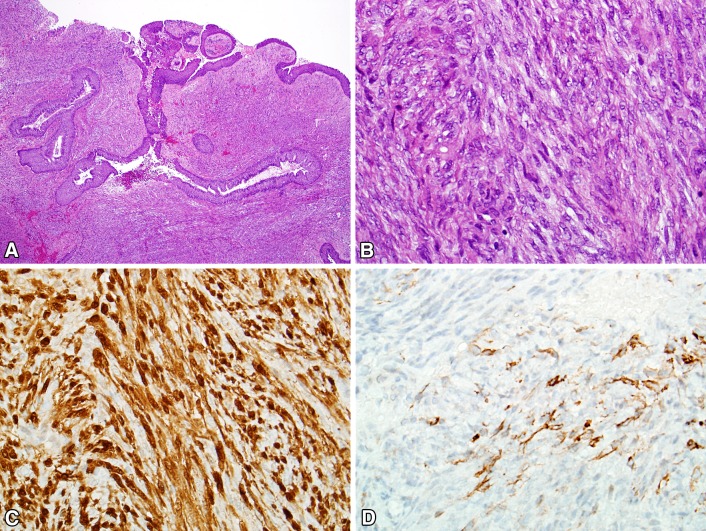
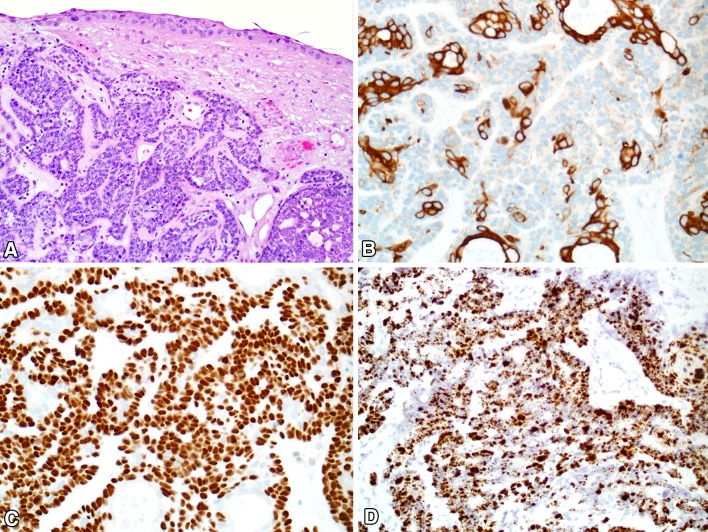
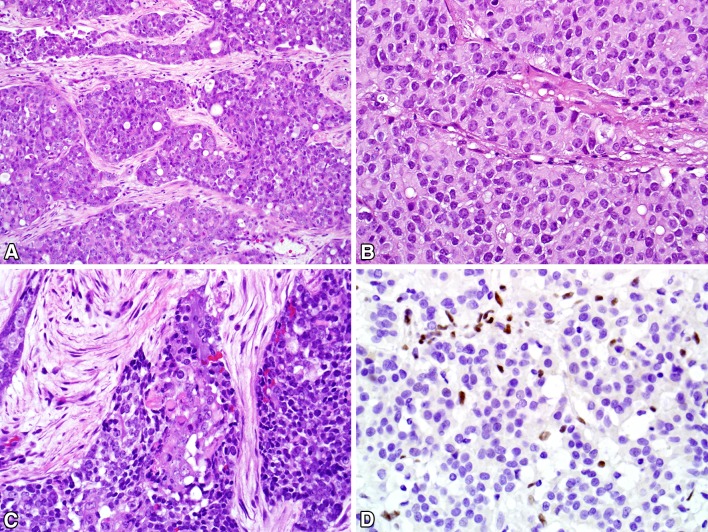
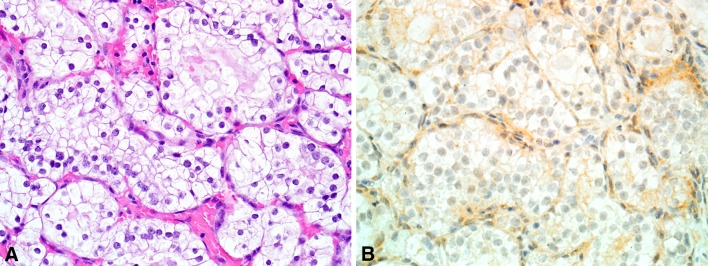
The sinonasal tract remains an epicenter of a diverse array of neoplasia. This paper discusses changes to the WHO classification system of tumors involving this area. In particular, seromucinous hamartoma, NUT carcinoma, biphenotypic sinonasal sarcoma, HPV-related carcinoma with adenoid cystic features, SMARCB1-deficient carcinoma, and renal cell-like adenocarcinoma are discussed.
Keywords: Adenoid cystic; Biphenotypical sinonasal sarcoma; Human papillomavirus; INI1; NUT carcinoma; Nasal; Seromucinous hamartoma; Sinonasal; Sinus; WHO.
Conflict of interest statement
Disclosure
Drs. Bishop and Stelow have no conflict of interest.
Research Involving Animal and Human Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
References
-
- Larque AB, Hakim S, Ordi J, Nadal A, Diaz A, del Pino M, Marimon L, Alobid I, Cardesa A, Alos L. High-risk human papillomavirus is transcriptionally active in a subset of sinonasal squamous cell carcinomas. Mod Pathol. 2014;27:343–351. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
