

Spontaneous Pneumothoraces in Patients with Birt-Hogg-Dubé Syndrome
- PMID: 28248571
- PMCID: PMC5427741
- DOI: 10.1513/AnnalsATS.201611-886OC
Spontaneous Pneumothoraces in Patients with Birt-Hogg-Dubé Syndrome
Abstract
Rationale: Spontaneous pneumothorax is a common complication of Birt-Hogg-Dubé syndrome (BHD).
Objectives: The optimal approach to treatment and prevention of BHD-associated spontaneous pneumothorax, and to advising patients with BHD regarding risk of pneumothorax associated with air travel, is not well established.
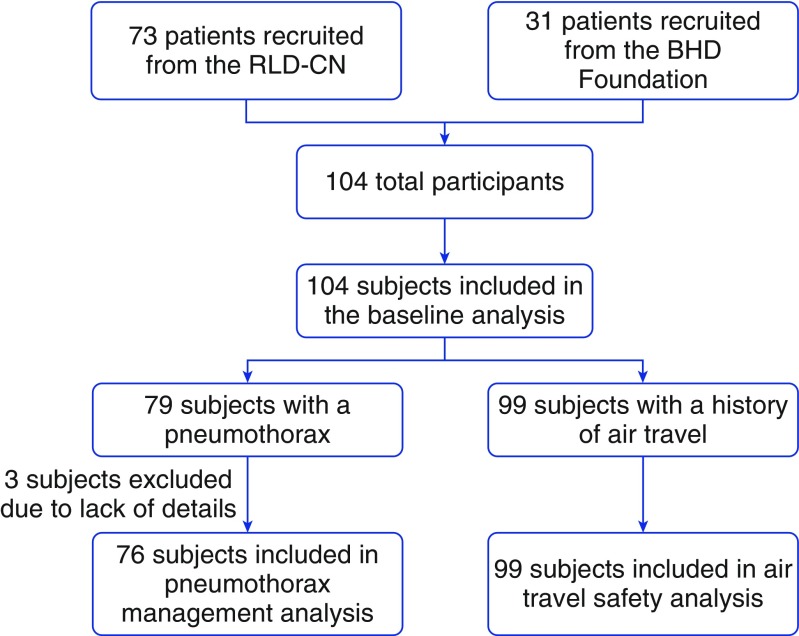
Methods: Patients with BHD were recruited from the Rare Lung Diseases Clinic Network and the BHD Foundation and surveyed about disease manifestations and air travel experiences.
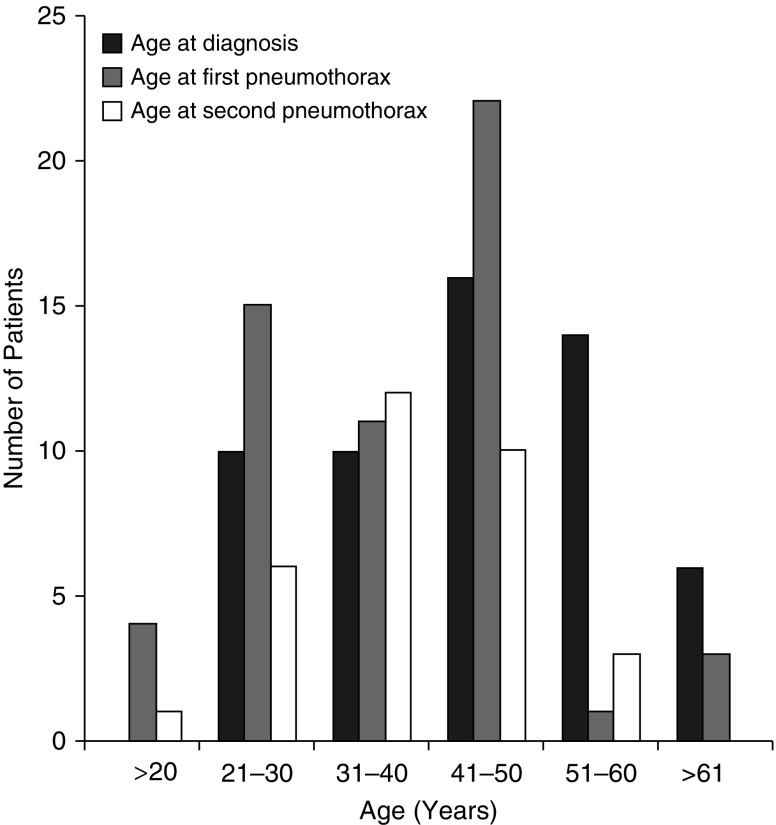
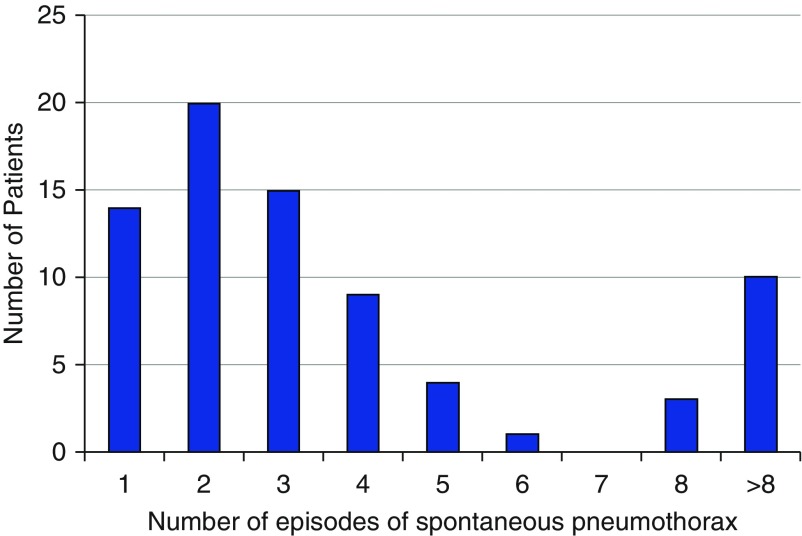
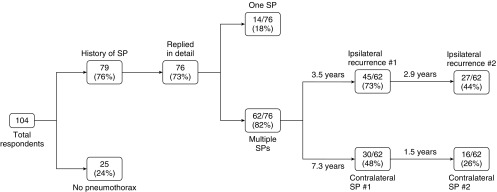
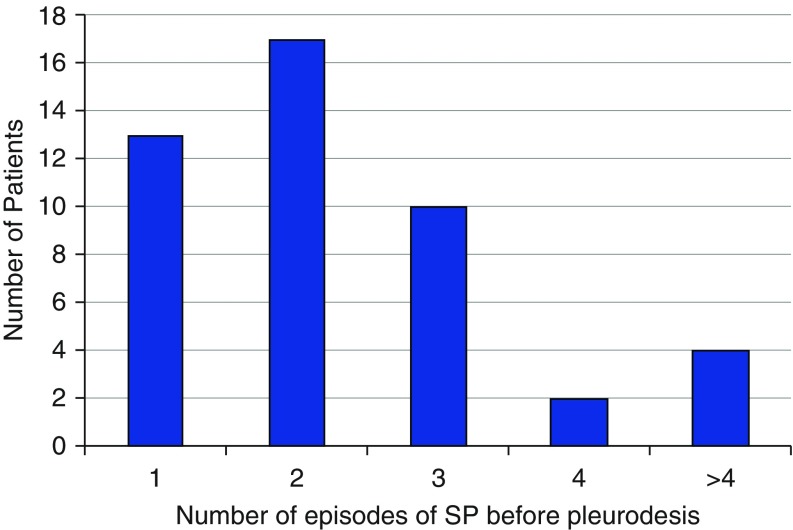
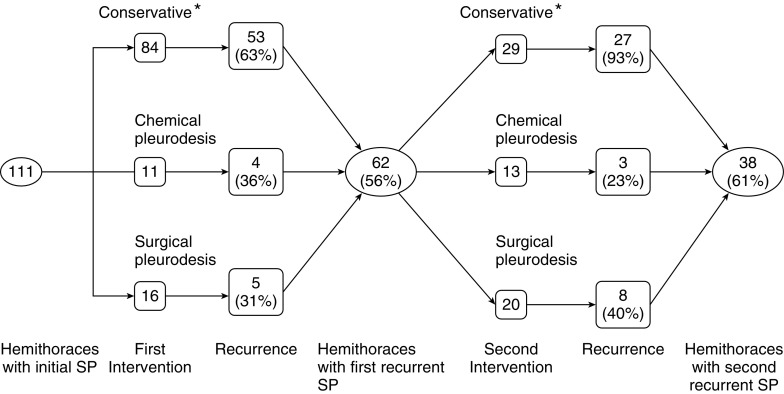
Results: A total of 104 patients completed the survey. The average age at diagnosis was 47 years, with an average delay from first symptoms of 13 years. Pulmonary cysts were the most frequent phenotypic manifestation of BHD, present in 85% of patients. Spontaneous pneumothorax was the presenting manifestation that led to the diagnosis of BHD in 65% of patients, typically after the second episode (mean, 2.4 episodes). Seventy-nine (76%) of 104 patients had at least one spontaneous pneumothorax during their lifetime, and 82% had multiple pneumothoraces. Among patients with multiple pneumothoraces, 73% had an ipsilateral recurrence, and 48% had a subsequent contralateral spontaneous pneumothorax following a sentinel event. The mean ages at first and second pneumothoraces were 36.5 years (range, 14-63 yr) and 37 years (range, 20-55 yr), respectively. The average number of spontaneous pneumothoraces experienced by patients with a sentinel pneumothorax was 3.6. Pleurodesis was generally performed after the second (mean, 2.4) ipsilateral pneumothorax and reduced the ipsilateral recurrence rate by half. A total of 11 episodes of spontaneous pneumothorax occurred among eight patients either during or within the 24-hour period following air travel, consistent with an air travel-related pneumothorax rate of 8% per patient and 0.12% per flight. Prior pleurodesis reduced the occurrence of a subsequent flight-related pneumothorax.
Conclusions: Spontaneous pneumothorax is an important, recurrent manifestation of pulmonary involvement in patients with BHD, and pleurodesis should be considered following the initial pneumothorax to reduce the risk of recurrent episodes. In general, in patients with BHD, pneumothorax occurs in about 1-2 per 1,000 flights, and the risk is lower among patients with a history of prior pleurodesis.
Keywords: Birt–Hogg–Dubé syndrome; air travel; pleurodesis; pneumothorax.
Figures
References
-
- Furuya M, Tanaka R, Koga S, Yatabe Y, Gotoda H, Takagi S, Hsu YH, Fujii T, Okada A, Kuroda N, et al. Pulmonary cysts of Birt-Hogg-Dubé syndrome: a clinicopathologic and immunohistochemical study of 9 families. Am J Surg Pathol. 2012;36:589–600. - PubMed
-
- Zbar B, Alvord WG, Glenn G, Turner M, Pavlovich CP, Schmidt L, Walther M, Choyke P, Weirich G, Hewitt SM, et al. Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev. 2002;11:393–400. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
