

Pathophysiology of Pediatric Multiple Organ Dysfunction Syndrome
- PMID: 28248832
- PMCID: PMC5333491
- DOI: 10.1097/PCC.0000000000001052
Pathophysiology of Pediatric Multiple Organ Dysfunction Syndrome
Abstract
Objective: To describe the pathophysiology associated with multiple organ dysfunction syndrome in children.
Data sources: Literature review, research data, and expert opinion.
Study selection: Not applicable.
Data extraction: Moderated by an experienced expert from the field, pathophysiologic processes associated with multiple organ dysfunction syndrome in children were described, discussed, and debated with a focus on identifying knowledge gaps and research priorities.
Data synthesis: Summary of presentations and discussion supported and supplemented by relevant literature.
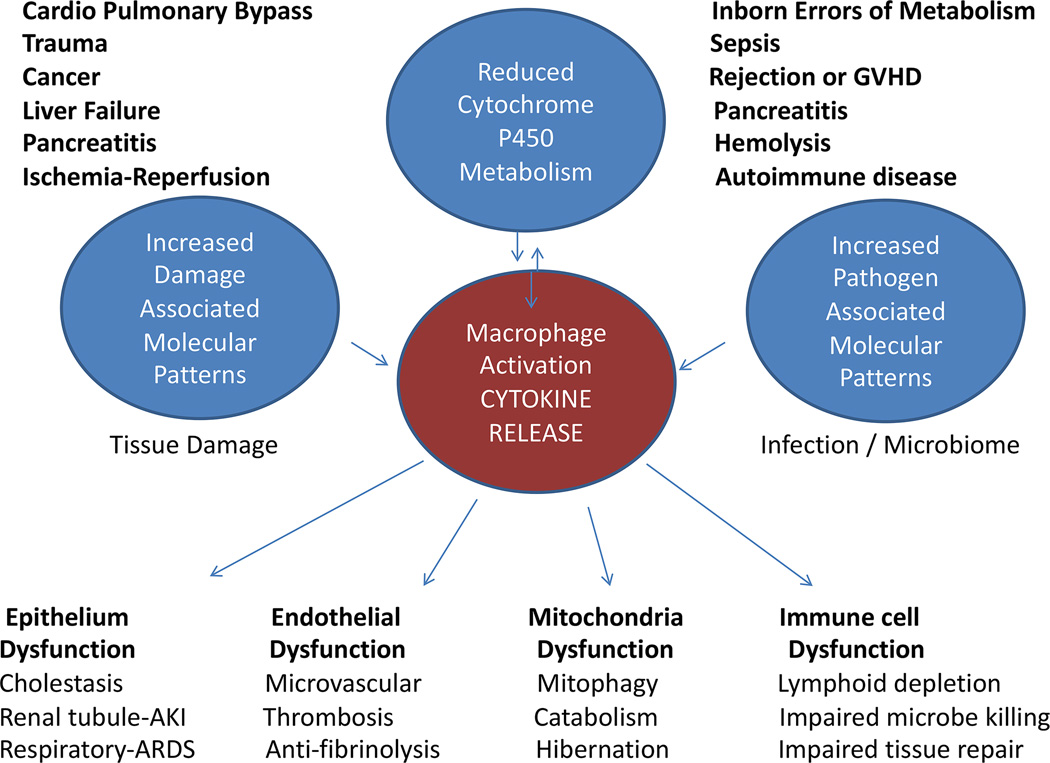
Conclusions: Experiment modeling suggests that persistent macrophage activation may be a pathophysiologic basis for multiple organ dysfunction syndrome. Children with multiple organ dysfunction syndrome have 1) reduced cytochrome P450 metabolism inversely proportional to inflammation; 2) increased circulating damage-associated molecular pattern molecules from injured tissues; 3) increased circulating pathogen-associated molecular pattern molecules from infection or endogenous microbiome; and 4) cytokine-driven epithelial, endothelial, mitochondrial, and immune cell dysfunction. Cytochrome P450s metabolize endogenous compounds and xenobiotics, many of which ameliorate inflammation, whereas damage-associated molecular pattern molecules and pathogen-associated molecular pattern molecules alone and together amplify the cytokine production leading to the inflammatory multiple organ dysfunction syndrome response. Genetic and environmental factors can impede inflammation resolution in children with a spectrum of multiple organ dysfunction syndrome pathobiology phenotypes. Thrombocytopenia-associated multiple organ dysfunction syndrome patients have extensive endothelial activation and thrombotic microangiopathy with associated oligogenic deficiencies in inhibitory complement and a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13. Sequential multiple organ dysfunction syndrome patients have soluble Fas ligand-Fas-mediated hepatic failure with associated oligogenic deficiencies in perforin and granzyme signaling. Immunoparalysis-associated multiple organ dysfunction syndrome patients have impaired ability to resolve infection and have associated environmental causes of lymphocyte apoptosis. These inflammation phenotypes can lead to macrophage activation syndrome. Resolution of multiple organ dysfunction syndrome requires elimination of the source of inflammation. Full recovery of organ functions is noted 6-18 weeks later when epithelial, endothelial, mitochondrial, and immune cell regeneration and reprogramming is completed.
Figures



References
-
- Baue AE. Multiple, progressive, or sequential systems failure. A syndrome of the 1970s. Arch Surg. 1975;110:779–781. - PubMed
-
- Baue AE. Recovery from multiple organ failure. Am J Surg. 1985;149:420–421. - PubMed
-
- Baue AE. Nutrition and metabolism in sepsis and multisystem organ failure. Surg Clin North Am. 1991;71:549–565. - PubMed
-
- Baue AE. The horror autotoxicus and multiple-organ failure. Arch Surg. 1992;127:1451–1462. - PubMed
-
- Chandel B, Shapiro MJ, Kurtz M, et al. MEGX (monoethylglycinexylidide): a novel in vivo test to measure early hepatic dysfunction after hypovolemic shock. Shock. 1995;3:51–53. discussion 54–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
