

Surgical strategies in the treatment of chronic pancreatitis: An updated systematic review and meta-analysis of randomized controlled trials
- PMID: 28248878
- PMCID: PMC5340451
- DOI: 10.1097/MD.0000000000006220
Surgical strategies in the treatment of chronic pancreatitis: An updated systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Chronic pancreatitis (CP) is a common and frequently occurring disease. Pancreaticoduodenectomy (PD), pylorus-preserving pancreaticoduodenectomy (PPPD), and duodenum-preserving pancreatic head resection (DPPHR) are important treatment options for patients with chronic pancreatitis. The Beger and Frey procedures are 2 main duodenum-preserving techniques in duodenum-preserving pancreatic head resection (DPPHR) strategies. We conducted this systematic review and meta-analysis to compare the clinical efficacy of DPPHR versus PD, the Beger procedure versus PD, the Frey procedure versus PD, and the Beger procedure versus the Frey procedure in the treatment of pancreatitis. The optimal surgical option for chronic pancreatitis is still under debate. The aim of this systematic review and meta-analysis was to evaluate the clinical efficacy of different surgical strategies for chronic pancreatitis.
Methods: Five databases (PubMed, Medline, SinoMed, Embase, and Cochrane Library) were searched with the limitations of human subjects and randomized controlled trials (RCTs) text. Data were extracted by 2 of the coauthors independently and analyzed using the RevMan statistical software, version 5.3. Weighted mean differences (WMDs), risk ratios (RRs), and 95% confidence intervals (CIs) were calculated. Cochrane Collaboration's Risk of Bias Tool was used to assess the risk of bias.
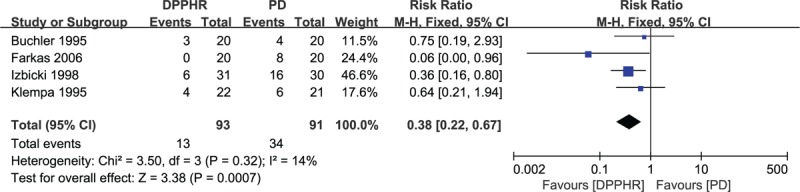
Results: Seven studies involving a total of 385 patients who underwent the surgical treatments were assessed. The methodological quality of the trials ranged from low to moderate and included PD (n = 134) and DPPHR (n = 251 [Beger procedure = 100; Frey procedure = 109; Beger or Frey procedure = 42]). There were no significant differences between DPPHR and PD in post-operation mortality (RR = 2.89, 95% CI = 0.31-26.87, P = 0.36), pain relief (RR = 1.09, 95% CI = 0.94-1.25, P = 0.26), exocrine insufficiency (follow-up time > 60 months: RR = 0.91, 95% CI = 0.72-1.15, P = 0.41), and endocrine insufficiency (RR = 0.75, 95% CI = 0.52-1.08, P = 0.12). Concerning the follow-up time < 60 months, the DPPHR group had better results of exocrine insufficiency (RR = 0.22, 95% CI = 0.08-0.62, P = 0.04). However, operation time (P < 0.0001), blood transfusion (P = 0.02), hospital stay (P = 0.0002), postoperation morbidity (P = 0.0007), weight gain (P < 0.00001), quality of life (P = 0.01), and occupational rehabilitation (P = 0.007) were significantly better for patients who underwent the DPPHR procedure compared with the PD procedure. The comparison results of the Frey procedure and PD showed that both procedures had an equal effect in the pain relief, postoperation mortality, exocrine and endocrine function, and quality of life (QoL) (P > 0.05), whereas patients who underwent the Frey procedure had significantly reduced operative times (P < 0.05) and less blood transfusions (P < 0.05). Comparing the Beger procedure to the PD procedure, there were no significant differences in hospital stay, blood transfusion, postoperation morbidity or mortality, pain relief, weight gain, exocrine insufficiency, and occupational rehabilitation (P > 0.05). Two studies comparing the Beger and Frey procedures showed no differences in postoperative morbidity, pain relief, exocrine insufficiency, and quality of life (P > 0.05). In terms of operative time, blood transfusion, hospital stay, postoperation morbidity, weight gain, quality of life, and occupational rehabilitation, the results also favored duodenum-preserving pancreatic head resection (DPPHR) strategies.
Conclusion: All procedures are equally effective for the management of pain, postoperation morbidity, exocrine insufficiency, and endocrine insufficiency for chronic pancreatitis. Improved short- and long-term outcomes, including operative time, blood transfusion, hospital stay, quality of life, weight gain, and occupational rehabilitation make DPPHR a more favorable surgical strategy for patients with chronic pancreatitis. Further, relevant trails are eager to prove these findings.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures















Similar articles
-
Duodenum-preserving pancreatic resection versus pancreaticoduodenectomy for chronic pancreatitis.Cochrane Database Syst Rev. 2016 Feb 3;2(2):CD011521. doi: 10.1002/14651858.CD011521.pub2. Cochrane Database Syst Rev. 2016. PMID: 26837472 Free PMC article.
-
Long-term Outcomes Favor Duodenum-preserving Pancreatic Head Resection over Pylorus-preserving Pancreaticoduodenectomy for Chronic Pancreatitis: A Meta-analysis and Systematic Review.Am Surg. 2015 Sep;81(9):909-14. Am Surg. 2015. PMID: 26350671
-
Duodenum-preserving pancreatic head resection versus pancreatoduodenectomy for surgical treatment of chronic pancreatitis: a systematic review and meta-analysis.Ann Surg. 2008 Jun;247(6):950-61. doi: 10.1097/SLA.0b013e3181724ee7. Ann Surg. 2008. PMID: 18520222
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Short and long-term post-operative outcomes of duodenum preserving pancreatic head resection for chronic pancreatitis affecting the head of pancreas: a systematic review and meta-analysis.HPB (Oxford). 2016 Feb;18(2):121-128. doi: 10.1016/j.hpb.2015.10.003. Epub 2015 Nov 17. HPB (Oxford). 2016. PMID: 26902130 Free PMC article.
Cited by
-
Comprehensive Outcomes of the Frey Procedure: A Single-center Perspective.Euroasian J Hepatogastroenterol. 2024 Jul-Dec;14(2):182-186. doi: 10.5005/jp-journals-10018-1445. Epub 2024 Dec 27. Euroasian J Hepatogastroenterol. 2024. PMID: 39802846 Free PMC article.
-
Long-term quality of life between duodenum-preserving pancreatic head resection and pancreatoduodenectomy: a systematic review and meta-analysis.Int J Surg. 2024 Feb 1;110(2):1139-1148. doi: 10.1097/JS9.0000000000000879. Int J Surg. 2024. PMID: 38000055 Free PMC article.
-
The Etiology of Pancreatic Manifestations in Patients with Inflammatory Bowel Disease.J Clin Med. 2019 Jun 26;8(7):916. doi: 10.3390/jcm8070916. J Clin Med. 2019. PMID: 31247968 Free PMC article. Review.
-
Surgical treatment of pain in chronic pancreatitis.Curr Opin Gastroenterol. 2018 Sep;34(5):317-321. doi: 10.1097/MOG.0000000000000460. Curr Opin Gastroenterol. 2018. PMID: 29901517 Free PMC article. Review.
-
Duodenum-preserving pancreatic head resection compared to pancreaticoduodenectomy: A systematic review and network meta-analysis of surgical outcomes.Front Surg. 2023 Mar 29;10:1107613. doi: 10.3389/fsurg.2023.1107613. eCollection 2023. Front Surg. 2023. PMID: 37066008 Free PMC article. Review.
References
-
- Braganza JM, Lee SH, McCloy RF, et al. Chronic pancreatitis. Lancet 2011;377:1184–97. - PubMed
-
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 2001;120:682–707. - PubMed
-
- Issa Y, Bruno MJ, Bakker OJ, et al. Treatment options for chronic pancreatitis. Nat Rev Gastroenterol Hepatol 2014;11:556–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
