

Pitfalls and Rewards for Implementing Ocular Motor Testing in Acute Vestibular Syndrome: A Pilot Project
- PMID: 28248913
- PMCID: PMC5334787
- DOI: 10.1097/NRL.0000000000000106
Pitfalls and Rewards for Implementing Ocular Motor Testing in Acute Vestibular Syndrome: A Pilot Project
Abstract
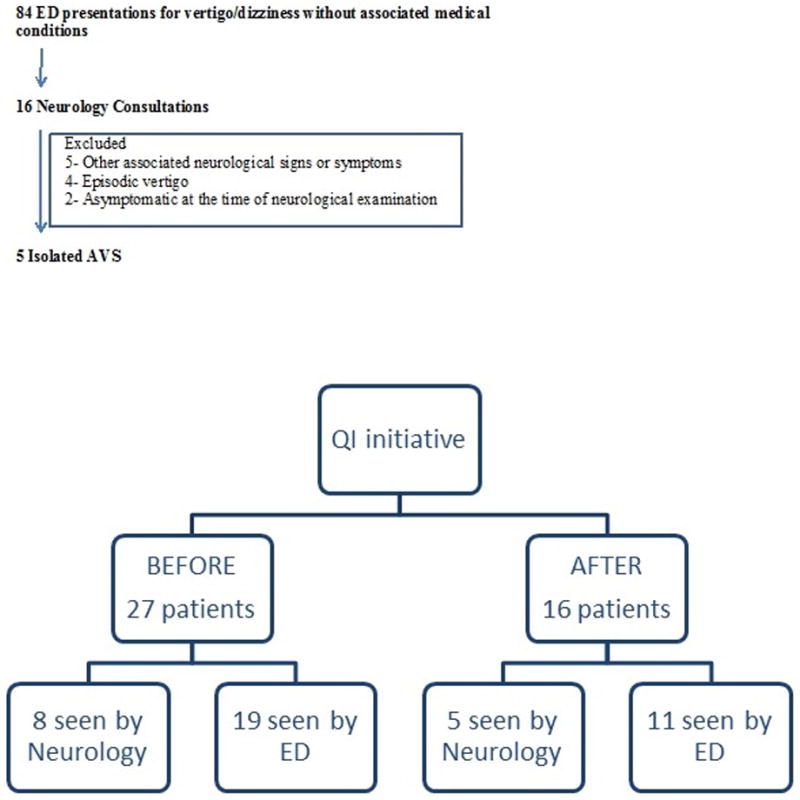
Objectives: Isolated acute vestibular syndrome (iAVS) presentations to the emergency department (ED) pose management challenges, given the concerns for posterior circulation strokes. False-negative brain imaging may erroneously reassure clinicians, whereas HINTS-plus examination outperforms imaging to screen for strokes in iAVS. We studied the feasibility of implementing HINTS-plus testing in the ED, aiming to reduce neuroimaging in patients with iAVS.
Methods: We launched an institutional Quality Improvement initiative, using DMAIC methodology. The outcome measures [proportion of iAVS subjects who had HINTS-plus examinations and underwent neuroimaging by computed tomography/magnetic resonance imaging (CT/MRI)] were compared before and after the established intervention. The intervention consisted of formal training for neurologists and emergency physicians on how to perform, document, and interpret HINTS-plus and implementation of novel iAVS management algorithm. Neuroimaging was not recommended if HINTS-plus suggested peripheral vestibular etiology. If a central process was suspected, brain MRI/MR angiogram was performed. Head CT was reserved only for thrombolytic time-window cases.
Results: In the first 2 months postimplementation, HINTS-plus testing performance by neurologists increased from 0% to 80% (P=0.007), and by ED providers from 0% to 9.09% (P=0.367). Head CT scans were reduced from 18.5% to 6.25%. Brain MRI use was reduced from 51.8% to 31.2%. About 60% of the iAVS subjects were discharged from the ED; none were readmitted or had another ED presentation in the ensuing 30 days.
Conclusions: Implementation of HINTS-plus evaluation in the ED is valuable and feasible for neurologists, but challenging for emergency physicians. Future studies should determine the "dose-response" curve of educational interventions.
Figures
Similar articles
-
HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness.Acad Emerg Med. 2013 Oct;20(10):986-96. doi: 10.1111/acem.12223. Acad Emerg Med. 2013. PMID: 24127701
-
Usage of the HINTS exam and neuroimaging in the assessment of peripheral vertigo in the emergency department.J Otolaryngol Head Neck Surg. 2018 Sep 10;47(1):54. doi: 10.1186/s40463-018-0305-8. J Otolaryngol Head Neck Surg. 2018. PMID: 30201056 Free PMC article.
-
Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms.Neurology. 2014 Jul 8;83(2):169-73. doi: 10.1212/WNL.0000000000000573. Epub 2014 Jun 11. Neurology. 2014. PMID: 24920847 Free PMC article.
-
Can Emergency Physicians Accurately Rule Out a Central Cause of Vertigo Using the HINTS Examination? A Systematic Review and Meta-analysis.Acad Emerg Med. 2020 Sep;27(9):887-896. doi: 10.1111/acem.13960. Epub 2020 Apr 8. Acad Emerg Med. 2020. PMID: 32167642
-
Diagnosing Stroke in Acute Vertigo: The HINTS Family of Eye Movement Tests and the Future of the "Eye ECG".Semin Neurol. 2015 Oct;35(5):506-21. doi: 10.1055/s-0035-1564298. Epub 2015 Oct 6. Semin Neurol. 2015. PMID: 26444396 Free PMC article. Review.
Cited by
-
Otoneurological evaluation: definitions and scientific evidence of bedside assessment and complementary exams. Outcomes of the II Brazilian Forum of Otoneurology.Braz J Otorhinolaryngol. 2025 May-Jun;91(3):101594. doi: 10.1016/j.bjorl.2025.101594. Epub 2025 May 13. Braz J Otorhinolaryngol. 2025. PMID: 40367707 Free PMC article. Review.
-
Acute vestibular migraine: a ghost diagnosis in patients with acute vertigo.J Neurol. 2023 Dec;270(12):6155-6158. doi: 10.1007/s00415-023-11930-9. Epub 2023 Aug 19. J Neurol. 2023. PMID: 37597072 No abstract available.
-
A Dynamic Nomogram to Predict the Risk of Stroke in Emergency Department Patients With Acute Dizziness.Front Neurol. 2022 Feb 18;13:839042. doi: 10.3389/fneur.2022.839042. eCollection 2022. Front Neurol. 2022. PMID: 35250839 Free PMC article.
-
The HINTS examination and STANDING algorithm in acute vestibular syndrome: A systematic review and meta-analysis involving frontline point-of-care emergency physicians.PLoS One. 2022 May 5;17(5):e0266252. doi: 10.1371/journal.pone.0266252. eCollection 2022. PLoS One. 2022. PMID: 35511910 Free PMC article.
-
Clinician's perspectives in using head impulse-nystagmus-test of skew (HINTS) for acute vestibular syndrome: UK experience.Stroke Vasc Neurol. 2022 Apr;7(2):172-175. doi: 10.1136/svn-2021-001229. Epub 2021 Oct 26. Stroke Vasc Neurol. 2022. PMID: 34702750 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
