

Cerebrospinal Fluid Shunting Complications in Children
- PMID: 28249297
- PMCID: PMC5915307
- DOI: 10.1159/000452840
Cerebrospinal Fluid Shunting Complications in Children
Abstract
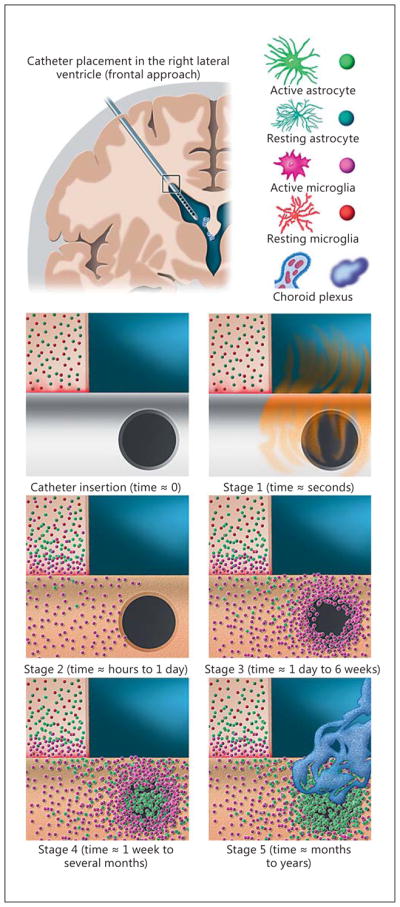
Although cerebrospinal fluid (CSF) shunt placement is the most common procedure performed by pediatric neurosurgeons, shunts remain among the most failure-prone life-sustaining medical devices implanted in modern medical practice. This article provides an overview of the mechanisms of CSF shunt failure for the 3 most commonly employed definitive CSF shunts in the practice of pediatric neurosurgery: ventriculoperitoneal, ventriculopleural, and ventriculoatrial. The text has been partitioned into the broad modes of shunt failure: obstruction, infection, mechanical shunt failure, overdrainage, and distal catheter site-specific failures. Clinical management strategies for the various modes of shunt failure are discussed as are research efforts directed towards reducing shunt complication rates. As it is unlikely that CSF shunting will become an obsolete procedure in the foreseeable future, it is incumbent on the pediatric neurosurgery community to maintain focused efforts to improve our understanding of and management strategies for shunt failure and shunt-related morbidity.
Keywords: Catheter obstruction; Hydrocephalus; Shunt failure; Ventriculoatrial shunt; Ventriculoperitoneal shunt; Ventriculopleural shunt.
© 2017 S. Karger AG, Basel.
Figures
References
-
- Browd SR, Ragel BT, Gottfried ON, Kestle JR. Failure of cerebrospinal fluid shunts: part I: obstruction and mechanical failure. Pediatr Neurol. 2006;34:83–92. - PubMed
-
- Kestle J, Drake J, Milner R, Sainte-Rose C, Cinalli G, Boop F, Piatt J, Haines S, Schiff S, Cochrane D, Steinbok P, MacNeil N. Long-term follow-up data from the Shunt Design Trial. Pediatr Neurosurg. 2000;33:230–236. - PubMed
-
- Riva-Cambrin J, Kestle JR, Holubkov R, Butler J, Kulkarni AV, Drake J, Whitehead WE, Wellons JC, Shannon CN, Tamber MS, Limbrick DD, Rozzelle C, Browd SR, Simon TD, Network HCR. Risk factors for shunt malfunction in pediatric hydrocephalus: a multi-center prospective cohort study. J Neurosurg Pediatr. 2016;17:382–390. - PubMed
-
- Pollack IF, Albright AL, Adelson PD. A randomized, controlled study of a programmable shunt valve versus a conventional valve for patients with hydrocephalus. Hakim-Medos Investigator Group. Neurosurgery. 1999;45:1399–1408. discussion 1408–1311. - PubMed
-
- Scott RM, Madsen JR. Shunt technology: contemporary concepts and prospects. Clin Neurosurg. 2003;50:256–267. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
