

Overdiagnosis of gastric cancer by endoscopic screening
- PMID: 28250897
- PMCID: PMC5311473
- DOI: 10.4253/wjge.v9.i2.55
Overdiagnosis of gastric cancer by endoscopic screening
Abstract
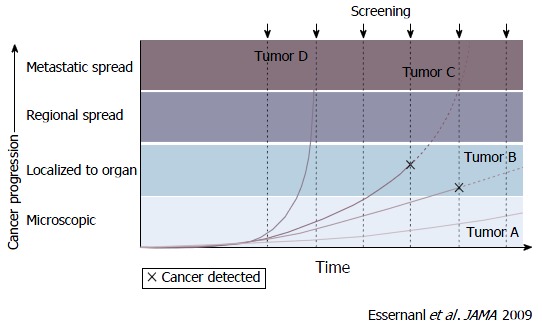
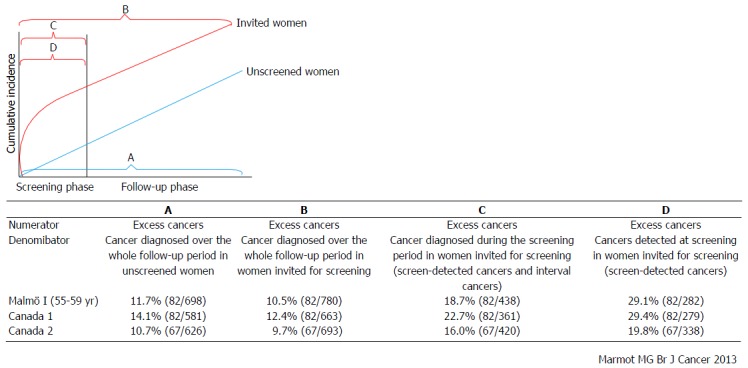
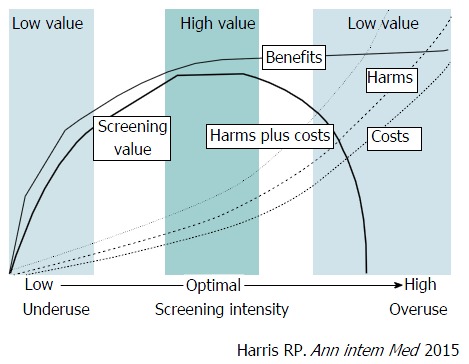
Gastric cancer screening using endoscopy has recently spread in Eastern Asian countries showing increasing evidence of its effectiveness. However, despite the benefits of endoscopic screening for gastric cancer, its major harms include infection, complications, false-negative results, false-positive results, and overdiagnosis. The most serious harm of endoscopic screening is overdiagnosis and this can occur in any cancer screening programs. Overdiagnosis is defined as the detection of cancers that would never have been found if there is no cancer screening. Overdiagnosis has been estimated from randomized controlled trials, observational studies, and modeling. It can be calculated on the basis of a comparison of the incidence of cancer between screened and unscreened individuals after the follow-up. Although the estimation method for overdiagnosis has not yet been standardized, estimation of overdiagnosis is needed in endoscopic screening for gastric cancer. To minimize overdiagnosis, the target age group and screening interval should be appropriately defined. Moreover, the balance of benefits and harms must be carefully considered to effectively introduce endoscopic screening in communities. Further research regarding overdiagnosis is warranted when evaluating the effectiveness of endoscopic screening.
Keywords: Cancer screening; Gastric cancer; Harm; Overdiagnosis; Upper gastrointestinal endoscopy.
Conflict of interest statement
Conflict-of-interest statement: The author has no conflicts of interest to report.
Figures

References
-
- Leung WK, Wu MS, Kakugawa Y, Kim JJ, Yeoh KG, Goh KL, Wu KC, Wu DC, Sollano J, Kachintorn U, et al. Screening for gastric cancer in Asia: current evidence and practice. Lancet Oncol. 2008;9:279–287. - PubMed
-
- Goto R, Hamashima C, Mun S, Lee WC. Why screening rates vary between Korea and Japan--differences between two national healthcare systems. Asian Pac J Cancer Prev. 2015;16:395–400. - PubMed
-
- Kim Y, Jun JK, Choi KS, Lee HY, Park EC. Overview of the National Cancer screening programme and the cancer screening status in Korea. Asian Pac J Cancer Prev. 2011;12:725–730. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
