

Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review
- PMID: 28251836
- PMCID: PMC5599950
- DOI: 10.1111/aos.13403
Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review
Abstract
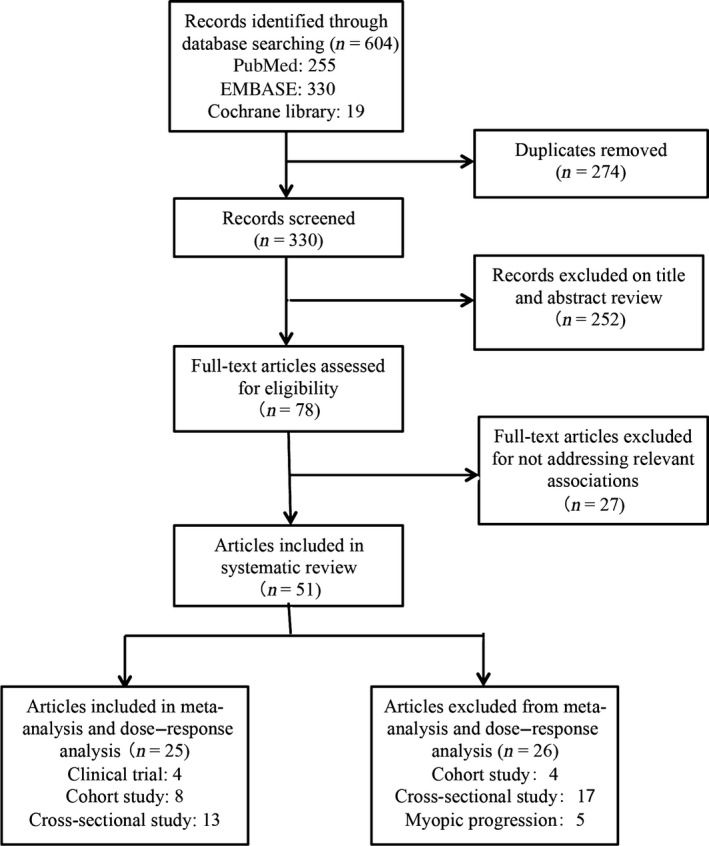
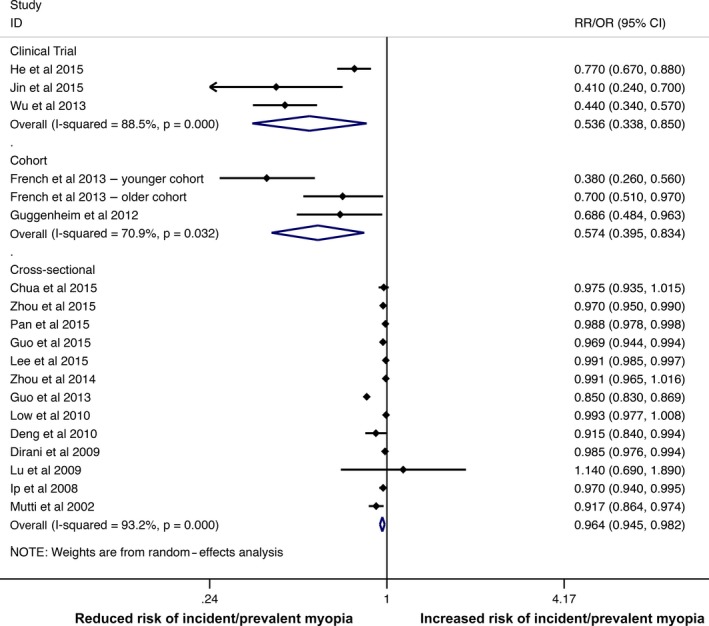
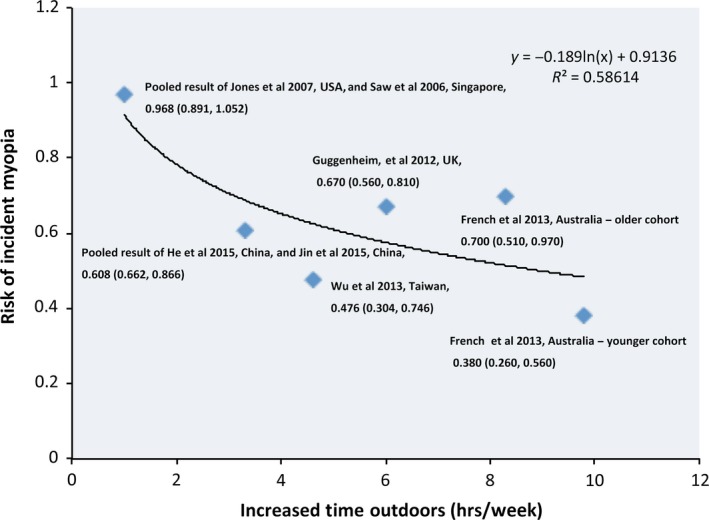
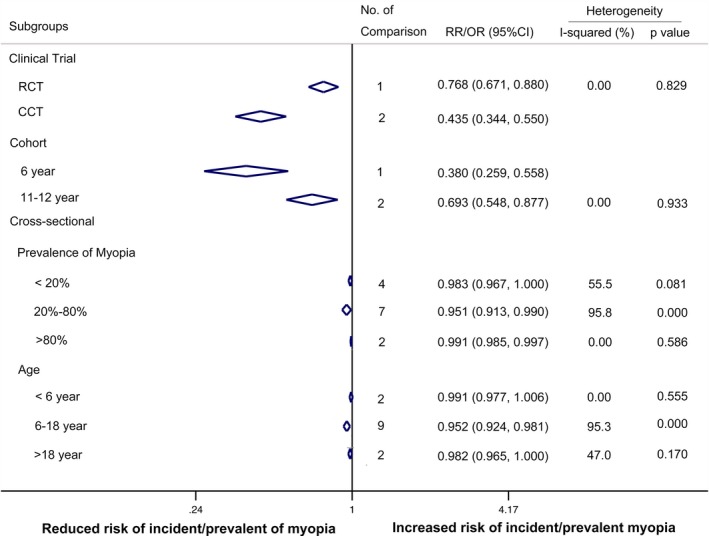
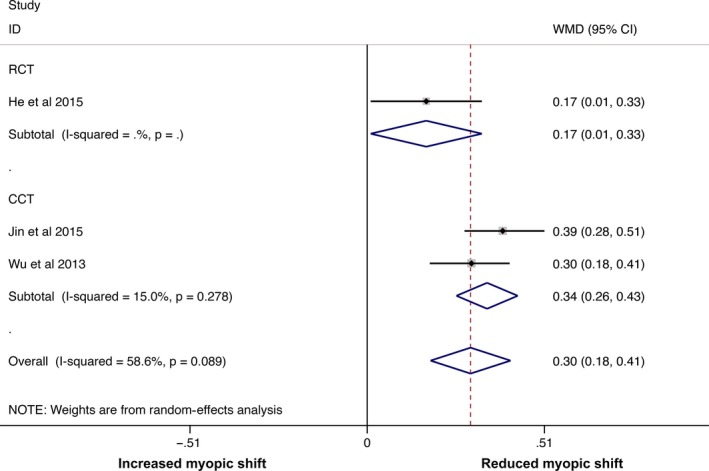
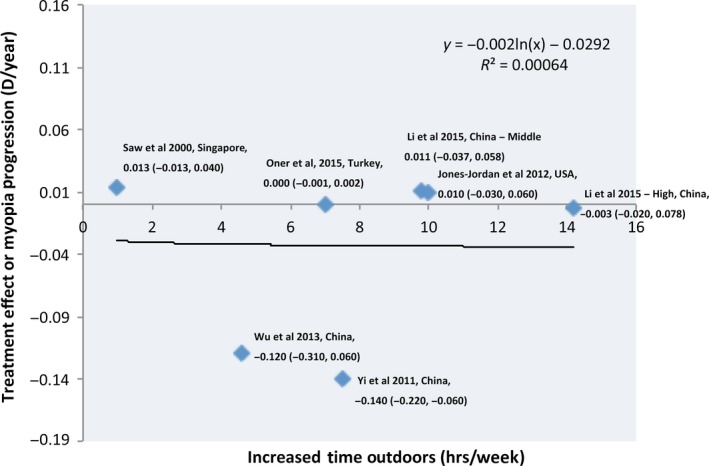
Outdoor time is considered to reduce the risk of developing myopia. The purpose is to evaluate the evidence for association between time outdoors and (1) risk of onset of myopia (incident/prevalent myopia); (2) risk of a myopic shift in refractive error and c) risk of progression in myopes only. A systematic review followed by a meta-analysis and a dose-response analysis of relevant evidence from literature was conducted. PubMed, EMBASE and the Cochrane Library were searched for relevant papers. Of the 51 articles with relevant data, 25 were included in the meta-analysis and dose-response analysis. Twenty-three of the 25 articles involved children. Risk ratio (RR) for binary variables and weighted mean difference (WMD) for continuous variables were conducted. Mantel-Haenszel random-effects model was used to pool the data for meta-analysis. Statistical heterogeneity was assessed using the I2 test with I2 ≥ 50% considered to indicate high heterogeneity. Additionally, subgroup analyses (based on participant's age, prevalence of myopia and study type) and sensitivity analyses were conducted. A significant protective effect of outdoor time was found for incident myopia (clinical trials: risk ratio (RR) = 0.536, 95% confidence interval (CI) = 0.338 to 0.850; longitudinal cohort studies: RR = 0.574, 95% CI = 0.395 to 0.834) and prevalent myopia (cross-sectional studies: OR = 0.964, 95% CI = 0.945 to 0.982). With dose-response analysis, an inverse nonlinear relationship was found with increased time outdoors reducing the risk of incident myopia. Also, pooled results from clinical trials indicated that when outdoor time was used as an intervention, there was a reduced myopic shift of -0.30 D (in both myopes and nonmyopes) compared with the control group (WMD = -0.30, 95% CI = -0.18 to -0.41) after 3 years of follow-up. However, when only myopes were considered, dose-response analysis did not find a relationship between time outdoors and myopic progression (R2 = 0.00064). Increased time outdoors is effective in preventing the onset of myopia as well as in slowing the myopic shift in refractive error. But paradoxically, outdoor time was not effective in slowing progression in eyes that were already myopic. Further studies evaluating effect of outdoor in various doses and objective measurements of time outdoors may help improve our understanding of the role played by outdoors in onset and management of myopia.
Keywords: dose-response analysis; meta-analysis; myopia; outdoor time.
© 2017 The Authors. Acta Ophthalmologica published by John Wiley & Sons Ltd on behalf of Acta Ophthalmologica Scandinavica Foundation.
Figures
References
-
- Bar Dayan Y, Levin A, Morad Y et al. (2005): The changing prevalence of myopia in young adults: a 13‐year series of population‐based prevalence surveys. Invest Ophthalmol Vis Sci 46: 2760–2765. - PubMed
-
- Chen C, Cheung SW & Cho P (2013): Myopia control using toric orthokeratology (TO‐SEE study). Invest Ophthalmol Vis Sci 54: 6510–6517. - PubMed
-
- Cheng CY, Huang W, Su KC, Peng ML, Sun HY & Cheng HM (2013): Myopization factors affecting urban elementary school students in Taiwan. Optom Vis Sci 90: 400–406. - PubMed
-
- Chia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A & Tan D (2012): Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 119: 347–354. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
