

Development and Prospective Validation of Tools to Accurately Identify Neurosurgical and Critical Care Events in Children With Traumatic Brain Injury
- PMID: 28252524
- PMCID: PMC5419849
- DOI: 10.1097/PCC.0000000000001120
Development and Prospective Validation of Tools to Accurately Identify Neurosurgical and Critical Care Events in Children With Traumatic Brain Injury
Abstract
Objective: To develop and validate case definitions (computable phenotypes) to accurately identify neurosurgical and critical care events in children with traumatic brain injury.
Design: Prospective observational cohort study, May 2013 to September 2015.
Setting: Two large U.S. children's hospitals with level 1 Pediatric Trauma Centers.
Patients: One hundred seventy-four children less than 18 years old admitted to an ICU after traumatic brain injury.
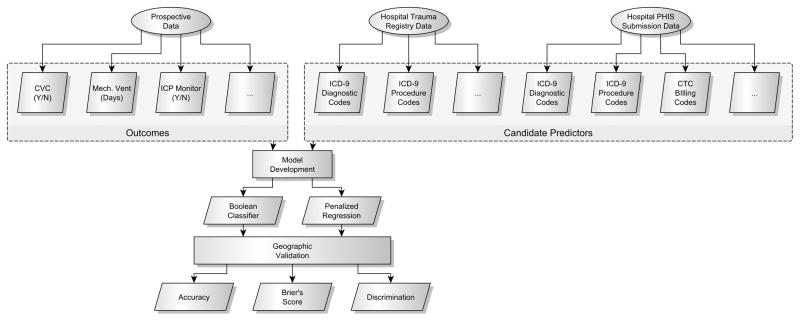
Measurements and main results: Prospective data were linked to database codes for each patient. The outcomes were prospectively identified acute traumatic brain injury, intracranial pressure monitor placement, craniotomy or craniectomy, vascular catheter placement, invasive mechanical ventilation, and new gastrostomy tube or tracheostomy placement. Candidate predictors were database codes present in administrative, billing, or trauma registry data. For each clinical event, we developed and validated penalized regression and Boolean classifiers (models to identify clinical events that take database codes as predictors). We externally validated the best model for each clinical event. The primary model performance measure was accuracy, the percent of test patients correctly classified. The cohort included 174 children who required ICU admission after traumatic brain injury. Simple Boolean classifiers were greater than or equal to 94% accurate for seven of nine clinical diagnoses and events. For central venous catheter placement, no classifier achieved 90% accuracy. Classifier accuracy was dependent on available data fields. Five of nine classifiers were acceptably accurate using only administrative data but three required trauma registry fields and two required billing data.
Conclusions: In children with traumatic brain injury, computable phenotypes based on simple Boolean classifiers were highly accurate for most neurosurgical and critical care diagnoses and events. The computable phenotypes we developed and validated can be used in any observational study of children with traumatic brain injury and can reasonably be applied in studies of these interventions in other patient populations.
Figures
Comment in
-
Why Everyone Should Care About "Computable Phenotypes".Pediatr Crit Care Med. 2017 May;18(5):489-490. doi: 10.1097/PCC.0000000000001115. Pediatr Crit Care Med. 2017. PMID: 28475533 Free PMC article. No abstract available.
References
-
- Faul M, Likang X, Wald M, et al. Traumatic brain injury in the united states: Emergency department visits, hospitalizations, and deaths 2002–2006. Atlanta (GA): National Center for Injury Prevention; Control, Centers for Disease Control; Prevention, U.S. Department of Health; Human Services; 2010.
-
- Kochanek PM, Carney N, Adelson PD, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents–second edition. Pediatr Crit Care Med. 2012;13(Suppl 1):S1–82. - PubMed
-
- Dreyer NA. Making observational studies count: Shaping the future of comparative effectiveness research. Epidemiology. 2011;22:295–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
