

Effects of pitavastatin and pravastatin on markers of immune activation and arterial inflammation in HIV
- PMID: 28252528
- PMCID: PMC5382495
- DOI: 10.1097/QAD.0000000000001427
Effects of pitavastatin and pravastatin on markers of immune activation and arterial inflammation in HIV
Abstract
Objective: Persistent immune activation is thought to contribute to increased cardiovascular disease risk in HIV and statins may help modulate systemic immune activation. We aimed to compare the effects of two key statins on markers of systemic immune activation and arterial inflammation in the HIV population.
Design: Double-blind, active-controlled, parallel-group comparative trial performed in 45 sites.
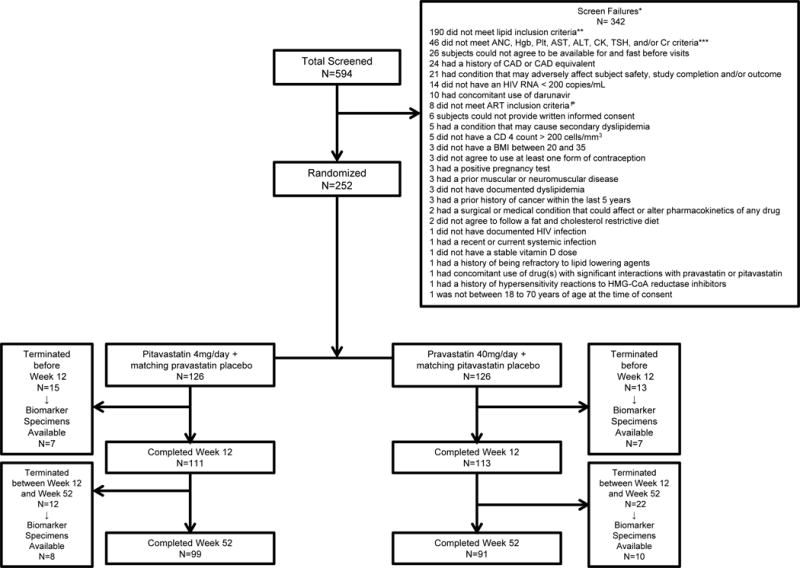
Methods: Two hundred and fifty-two antiretroviral therapy-treated HIV-infected participants with dyslipidemia were randomized (1 : 1) to pitavastatin 4 mg daily vs. pravastatin 40 mg daily in the HIV-infected patieNts and TREatment with PItavastatin vs. pravastatin for Dyslipidemia (INTREPID) trial. In this analysis of the INTREPID trial, we assessed markers of immune activation and arterial inflammation using a modified intent-to-treat population. This trial is registered with ClinicalTrials.gov (NCT01301066).
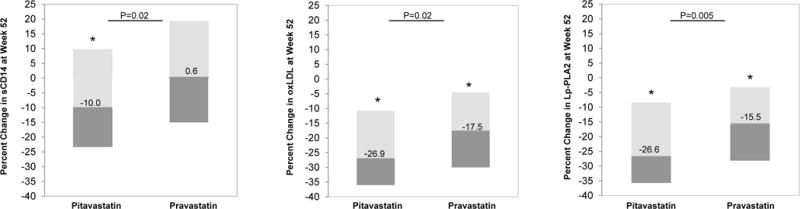
Results: One hundred and twenty-six participants were randomized to receive pitavastatin and 126 to pravastatin. Ninety-nine participants in the pitavastatin group and 91 participants in the pravastatin group completed the study. Median age was 50 (45, 56) years [median (interquartile range)]. Baseline, low-density lipoprotein-cholestrol (LDL-C) was 153 (135, 171) mg/dl, log HIV-1 viral load was 1.1 ± 0.2 copies/ml, and CD4 cell count was 580 (439, 794) cells/μl. At week 52, the pitavastatin group had a significantly greater reduction (% change) compared with pravastatin in soluble CD14 (sCD14), (-10.0 vs. 0.6%, P = 0.02), oxidized LDL (oxLDL) (-26.9 vs. -17.5%, P = 0.02), and lipoprotein-associated phospholipase 2 (Lp-PLA2) (-26.6 vs. -15.5%, P = 0.005) (pitavastatin vs. pravastatin).
Conclusion: Fifty-two weeks of pitavastatin 4 mg daily (vs. pravastatin 40 mg daily) led to a greater reduction in select markers of immune activation and arterial inflammation (sCD14, oxLDL, and LpPLA2) among HIV-infected participants. Further work is needed to assess whether immune-modulatory effects of pitavastatin reduce cardiovascular disease risk in HIV.
Conflict of interest statement
KCW served on the scientific advisory board and was paid by Macrophage Therapeutics LLC, unrelated to this study. CAS and MMP are employees of KOWA Pharmaceuticals America, Inc. JAA received grants from KOWA Pharmaceuticals America, Inc during the conduct of the study, served in scientific advisory board personal from Janssen, Merck, and ViiV Healthcare, and received grants from Bristol-Myers Squibb and Gilead Sciences. MVZ participated in a scientific advisory board meeting for Roche Diagnostics and received grant support from Gilead Sciences, both unrelated to this study. SKG served as a paid consultant to Gilead Sciences, Theratechnologies, BMS, NovoNordisk, Merck, Navidea, and AstraZeneca and received grant support from Amgen, BMS, Gilead Sciences, KOWA Pharmaceuticals America, Inc and Theratechnologies unrelated to this study. SKG also received a grant to perform this project from KOWA Pharmaceuticals America, Inc. No other competing interests were reported.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
