

Longitudinal sampling of the lung microbiota in individuals with cystic fibrosis
- PMID: 28253277
- PMCID: PMC5333848
- DOI: 10.1371/journal.pone.0172811
Longitudinal sampling of the lung microbiota in individuals with cystic fibrosis
Abstract
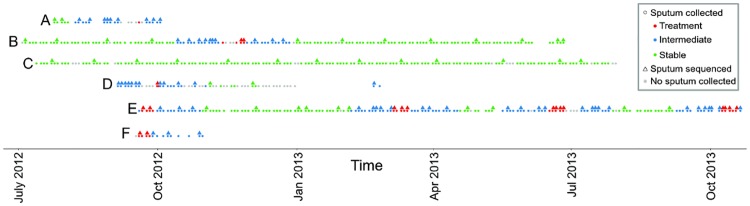
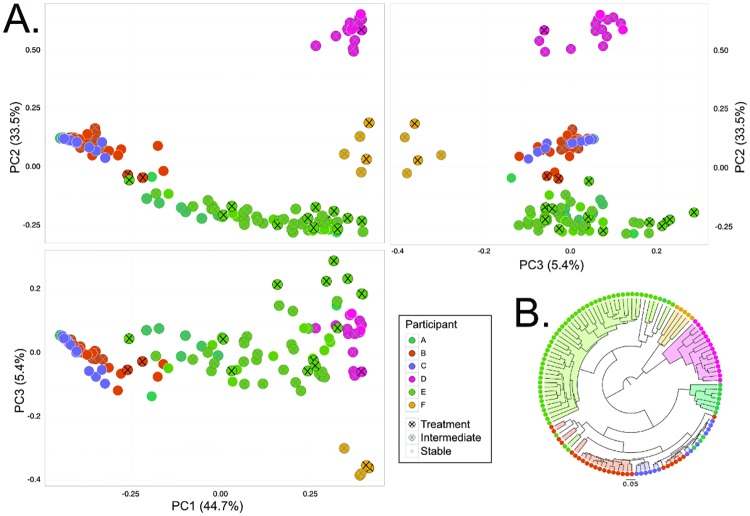
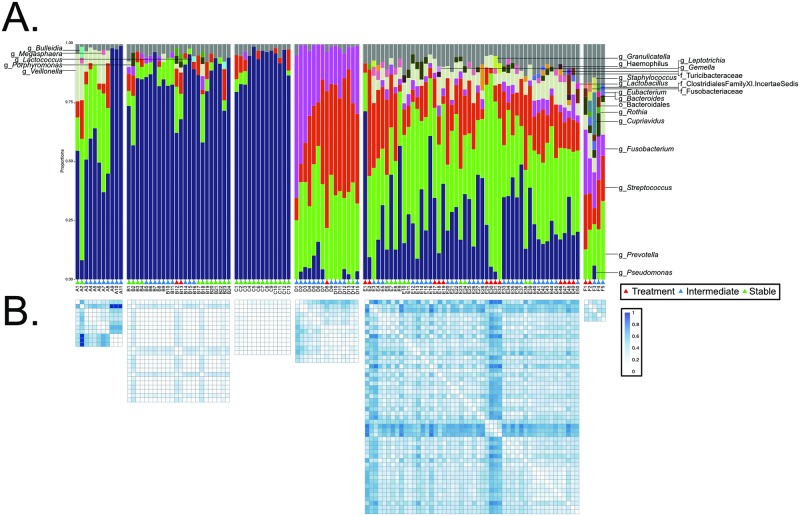
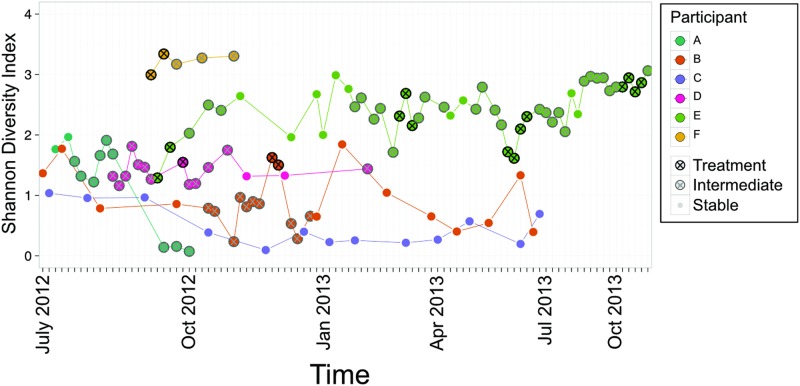
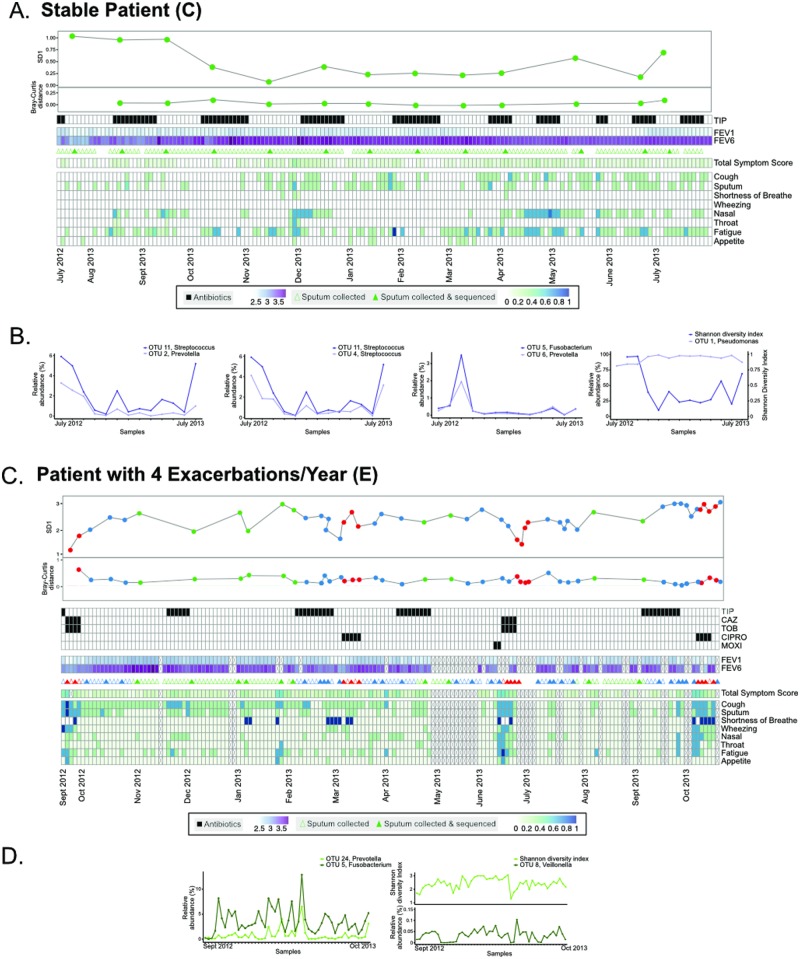
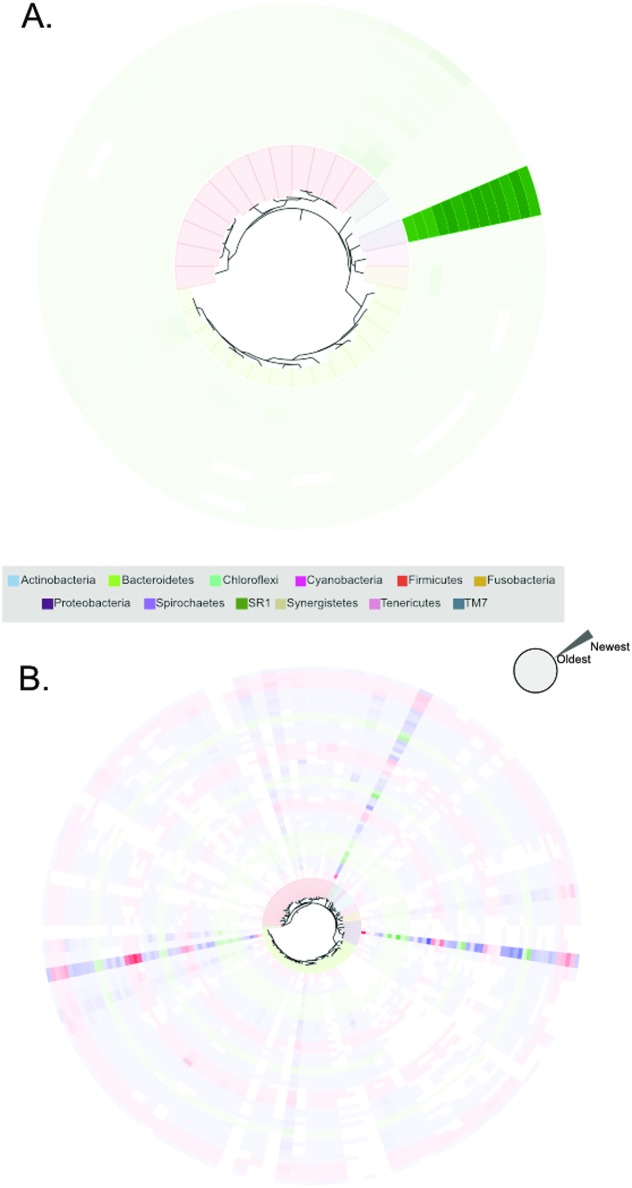
Cystic fibrosis (CF) manifests in the lungs resulting in chronic microbial infection. Most morbidity and mortality in CF is due to cycles of pulmonary exacerbations-episodes of acute inflammation in response to the lung microbiome-which are difficult to prevent and treat because their cause is not well understood. We hypothesized that longitudinal analyses of the bacterial component of the CF lung microbiome may elucidate causative agents within this community for pulmonary exacerbations. In this study, 6 participants were sampled thrice-weekly for up to one year. During sampling, sputum, and data (antibiotic usage, spirometry, and symptom scores) were collected. Time points were categorized based on relation to exacerbation as Stable, Intermediate, and Treatment. Retrospectively, a subset of were interrogated via 16S rRNA gene sequencing. When samples were examined categorically, a significant difference between the lung microbiota in Stable, Intermediate, and Treatment samples was observed in a subset of participants. However, when samples were examined longitudinally, no correlations between microbial composition and collected data (antibiotic usage, spirometry, and symptom scores) were observed upon exacerbation onset. In this study, we identified no universal indicator within the lung microbiome of exacerbation onset but instead showed that changes to the CF lung microbiome occur outside of acute pulmonary episodes and are patient-specific.
Conflict of interest statement
Figures
Similar articles
-
The adult cystic fibrosis airway microbiota is stable over time and infection type, and highly resilient to antibiotic treatment of exacerbations.PLoS One. 2012;7(9):e45001. doi: 10.1371/journal.pone.0045001. Epub 2012 Sep 26. PLoS One. 2012. PMID: 23049765 Free PMC article.
-
Impact of Anaerobic Antibacterial Spectrum on Cystic Fibrosis Airway Microbiome Diversity and Pulmonary Function.Pediatr Infect Dis J. 2021 Nov 1;40(11):962-968. doi: 10.1097/INF.0000000000003211. Pediatr Infect Dis J. 2021. PMID: 34269323 Free PMC article.
-
The effects of cycled inhaled aztreonam on the cystic fibrosis (CF) lung microbiome.J Cyst Fibros. 2019 Nov;18(6):829-837. doi: 10.1016/j.jcf.2019.02.010. Epub 2019 Mar 8. J Cyst Fibros. 2019. PMID: 30857926
-
Microbiome in the pathogenesis of cystic fibrosis and lung transplant-related disease.Transl Res. 2017 Jan;179:84-96. doi: 10.1016/j.trsl.2016.07.022. Epub 2016 Aug 4. Transl Res. 2017. PMID: 27559681 Review.
-
Cystic fibrosis lung microbiome: opportunities to reconsider management of airway infection.Pediatr Pulmonol. 2015 Oct;50 Suppl 40:S31-8. doi: 10.1002/ppul.23243. Pediatr Pulmonol. 2015. PMID: 26335953 Review.
Cited by
-
Is there a role for antibiotics in the treatment of chronic rhinosinusitis?J Allergy Clin Immunol. 2022 May;149(5):1504-1512. doi: 10.1016/j.jaci.2022.02.004. Epub 2022 Feb 22. J Allergy Clin Immunol. 2022. PMID: 35217148 Free PMC article. Review.
-
Cystic fibrosis respiratory microbiota: unraveling complexity to inform clinical practice.Expert Rev Respir Med. 2018 Oct;12(10):857-865. doi: 10.1080/17476348.2018.1513331. Epub 2018 Sep 3. Expert Rev Respir Med. 2018. PMID: 30118374 Free PMC article. Review.
-
Clinical practices underlie COVID-19 patient respiratory microbiome composition and its interactions with the host.Nat Commun. 2021 Oct 29;12(1):6243. doi: 10.1038/s41467-021-26500-8. Nat Commun. 2021. PMID: 34716338 Free PMC article.
-
The Epithelial-Immune Crosstalk in Pulmonary Fibrosis.Front Immunol. 2021 May 19;12:631235. doi: 10.3389/fimmu.2021.631235. eCollection 2021. Front Immunol. 2021. PMID: 34093523 Free PMC article. Review.
-
Untargeted Metagenomic Investigation of the Airway Microbiome of Cystic Fibrosis Patients with Moderate-Severe Lung Disease.Microorganisms. 2020 Jul 4;8(7):1003. doi: 10.3390/microorganisms8071003. Microorganisms. 2020. PMID: 32635564 Free PMC article.
References
-
- Kerem B, Rommens JM, Buchanan JA, Markiewicz D, Cox TK, Chakravarti A, et al. Identification of the cystic fibrosis gene: genetic analysis. Science [Internet]. 1989. September 8 [cited 2016 Aug 1];245(4922):1073–80. Available from: http://www.ncbi.nlm.nih.gov/pubmed/2570460 - PubMed
-
- O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet [Internet]. Elsevier; 2009. May 30 [cited 2014 Jul 9];373(9678):1891–904. Available from: http://www.thelancet.com/article/S0140673609603275/fulltext - PubMed
-
- Elborn JS. Cystic fibrosis. Lancet (London, England) [Internet]. 2016 Apr 29 [cited 2016 May 4]; http://www.ncbi.nlm.nih.gov/pubmed/27140670
-
- ANDERSEN DH, Holt LE. and H J, Göttche O, Landsteiner K, Kornblith BA. and O S, Passini F, et al. CYSTIC FIBROSIS OF THE PANCREAS AND ITS RELATION TO CELIAC DISEASE. Am J Dis Child [Internet]. American Medical Association; 1938. August 1 [cited 2016 Aug 1];56(2):344 Available from: http://archpedi.jamanetwork.com/article.aspx?doi=10.1001/archpedi.1938.0...
-
- Ferkol T, Rosenfeld M, Milla CE. Cystic fibrosis pulmonary exacerbations. J Pediatr [Internet]. 2006. February [cited 2015 Jul 14];148(2):259–64. Available from: http://www.sciencedirect.com/science/article/pii/S0022347605010073 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
