

A relationship to survival is seen by combining the factors of mismatch repair status, tumor location and age of onset in colorectal cancer patients
- PMID: 28253296
- PMCID: PMC5333840
- DOI: 10.1371/journal.pone.0172799
A relationship to survival is seen by combining the factors of mismatch repair status, tumor location and age of onset in colorectal cancer patients
Abstract
Background: The progression of colorectal cancer (CRC) may differ depending on the location of the tumor and the age of onset of the disease. Previous studies also suggested that the molecular basis of CRC varies with tumor location, which could affect the clinical management of patients. Therefore, we performed survival analysis looking at different age groups and mismatch repair status (MMR) of CRC patients according to primary tumor location in an attempt to identify subgroups of CRC that might help in the prognosis of disease.
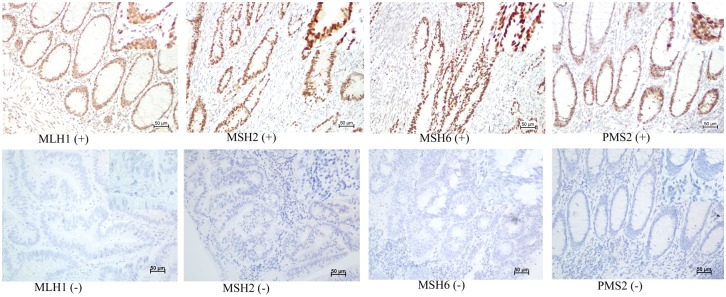
Methods: A group of 2233 patients operated on to remove their CRC tumors were analyzed (521 with right colon cancer, 740 with left colon cancer and 972 with rectal cancer). The expression of four MMR genes was assessed by immunohistochemistry (IHC), independent of clinical criteria. From the data collected, a predictive model for overall survival (OS) could be constructed for some associations of tumor location and age of onset using Kaplan-Meier, logistic and Cox regression analysis.
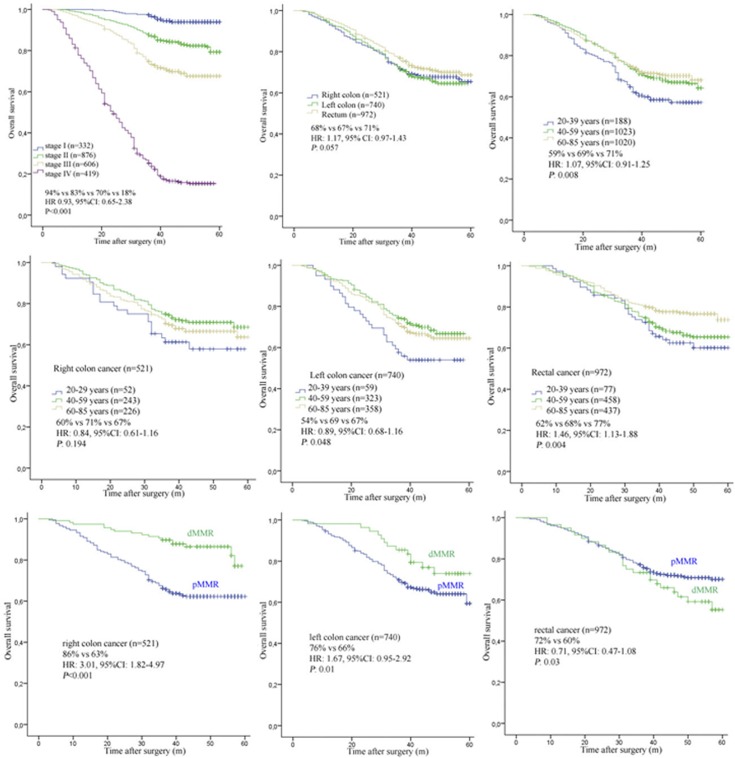
Results: When tumor location was considered as the lone factor, we found no statistical difference in overall survival (OS) between right cancer (68%), left cancer (67%) or rectal cancer tumor locations (71%) (HR: 1.17, 95%CI (confidence interval): 0.97-1.43, P = 0.057). When age of onset was considered, middle age (40-59 years) and older (60-85 years) patients were found to have higher OS than younger onset cancer (20-39 years) patients (69% vs 71% vs 59%, HR: 1.07, 95% confidence interval (CI): 0.91-1.25, P = 0.008). When both age of onset and tumor location were considered in combination as disease factors, we found that the subgroup of patients with left colon cancer from middle age (69%) and older (67%) aged patients had higher OS than younger (54%) patients (HR: 0.89, 95%CI: 0.68-1.16, P = 0.048). However in patients with right colon cancers, we found no statistical difference is OS between younger, middle age or older grouped patients (60% vs 71% vs 67%, HR: 0.84, 95% CI: 0.61-1.16, P = 0.194). With regard to rectal located cancers, we found that younger (62%) and middle age (68) patients had lower OS than older (77%) patients (HR:1.46, 95%CI: 1.13-1.88, P = 0.004). The rates of deficient MMR (dMMR) was 10.4%. We found no statistical difference in OS stratified by tumor locations. However, right colon cancer patients with dMMR (86%) had higher OS than those with proficient MMR (pMMR) (63%) (HR: 3.01, 95% CI: 1.82-4.97, P<0.001). Left colon cancer patients with dMMR (76%) also had higher OS than those with pMMR (66%) (HR: 1.67, 95% CI: 0.95-2.92, P = 0.01). Oppositely, rectal cancer patients with dMMR (60%) had lower OS than those pMMR (68%) (HR: 0.77, 95% CI: 0.51-1.17, P = 0.04).
Conclusions: These data demonstrate that primary tumor location can be an important factor when considered along with age of onset for the prognosis of CRC. Primary tumor location is also an important factor to evaluate the predictive effect of MMR status for the prognosis of CRC.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
