

Salivary inflammatory markers and microbiome in normoglycemic lean and obese children compared to obese children with type 2 diabetes
- PMID: 28253297
- PMCID: PMC5333807
- DOI: 10.1371/journal.pone.0172647
Salivary inflammatory markers and microbiome in normoglycemic lean and obese children compared to obese children with type 2 diabetes
Erratum in
-
Correction: Salivary inflammatory markers and microbiome in normoglycemic lean and obese children compared to obese children with type 2 diabetes.PLoS One. 2017 Aug 16;12(8):e0183600. doi: 10.1371/journal.pone.0183600. eCollection 2017. PLoS One. 2017. PMID: 28813516 Free PMC article.
Abstract
Background: There is emerging evidence linking diabetes with periodontal disease. Diabetes is a well-recognized risk factor for periodontal disease. Conversely, pro-inflammatory molecules released by periodontally-diseased tissues may enter the circulation to induce insulin resistance. While this association has been demonstrated in adults, there is little information regarding periodontal status in obese children with and without type 2 diabetes (T2D). We hypothesized that children with T2D have higher rates of gingivitis, elevated salivary inflammatory markers, and an altered salivary microbiome compared to children without T2D.
Methods: Three pediatric cohorts ages 10-19 years were studied: lean (normal weight-C), obese (Ob), and obese with T2D (T2D). Each subject completed an oral health survey, received a clinical oral examination, and provided unstimulated saliva for measurement of inflammatory markers and microbiome analysis.
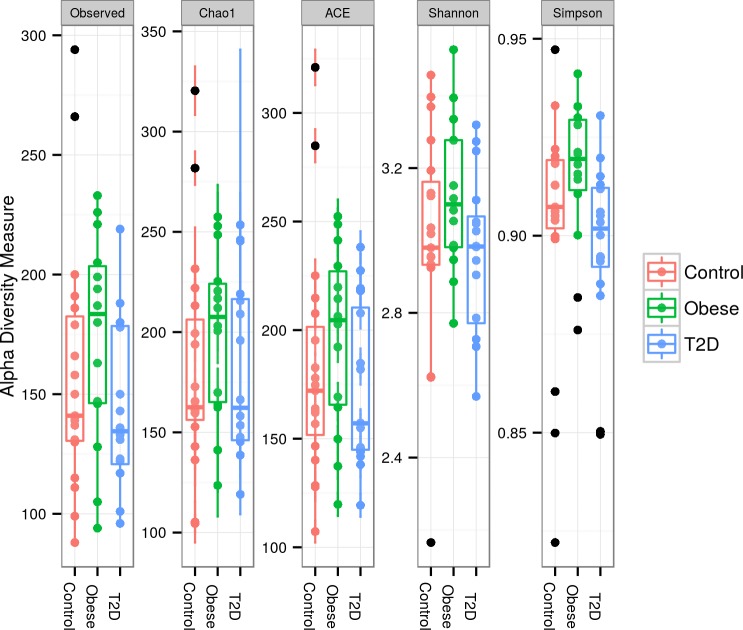
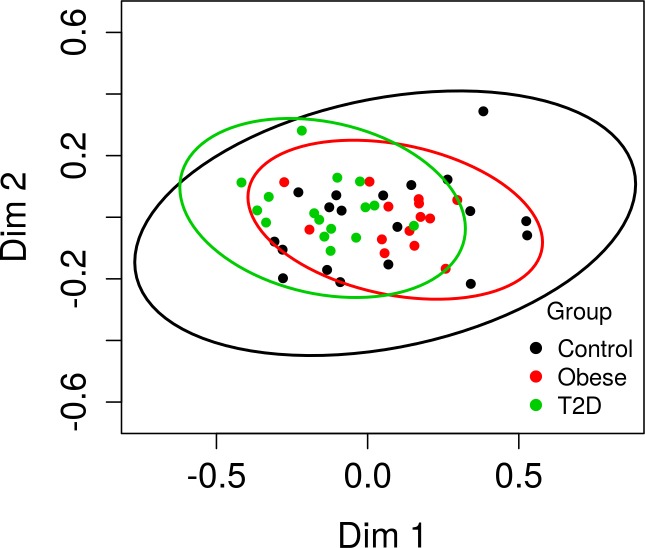
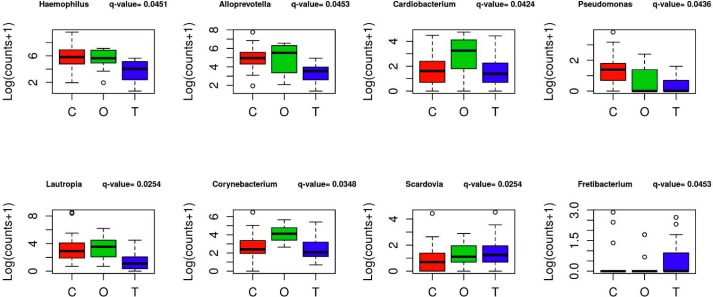
Results: The diabetes group was less likely to have had a dental visit within the last six months. Body mass index (BMI) Z-scores and waist circumference/height ratios were similar between Ob and T2D cohorts. The number of carious lesions and fillings were similar for all three groups. The gingival index was greater in the T2D group compared to the Ob and C groups. Although salivary microbial diversity was minimal between groups, a few differences in bacterial genus composition were noted.
Conclusions: Obese children with T2D show a trend toward poorer oral health compared to normal weight and obese children without T2D. This study characterizes the salivary microbiome of children with and without obesity and T2D. This study supports a modest link between T2D and periodontal inflammation in the pediatric population.
Conflict of interest statement
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
