

Effect of goal-directed therapy on outcome after esophageal surgery: A quality improvement study
- PMID: 28253353
- PMCID: PMC5333843
- DOI: 10.1371/journal.pone.0172806
Effect of goal-directed therapy on outcome after esophageal surgery: A quality improvement study
Abstract
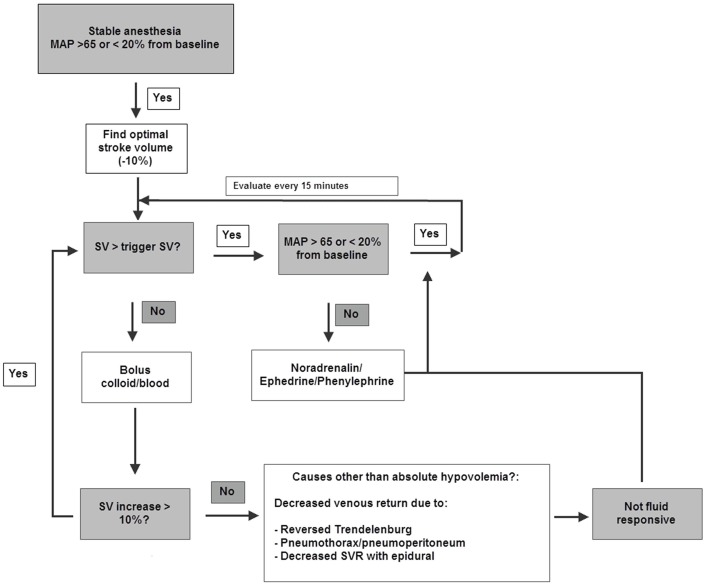
Background: Goal-directed therapy (GDT) can reduce postoperative complications in high-risk surgery patients. It is uncertain whether GDT has the same benefits in patients undergoing esophageal surgery. Goal of this Quality Improvement study was to evaluate the effects of a stroke volume guided GDT on post-operative outcome.
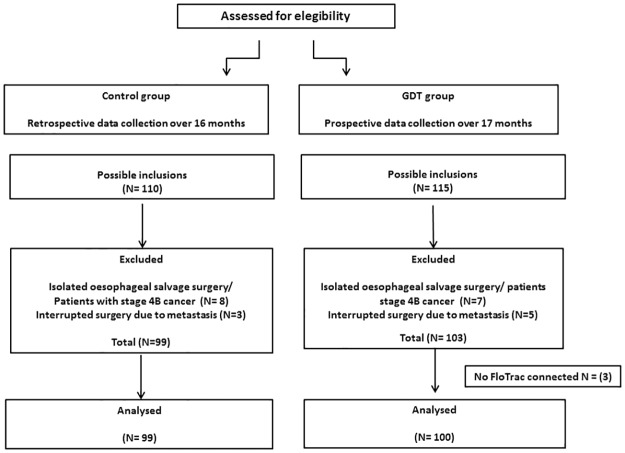
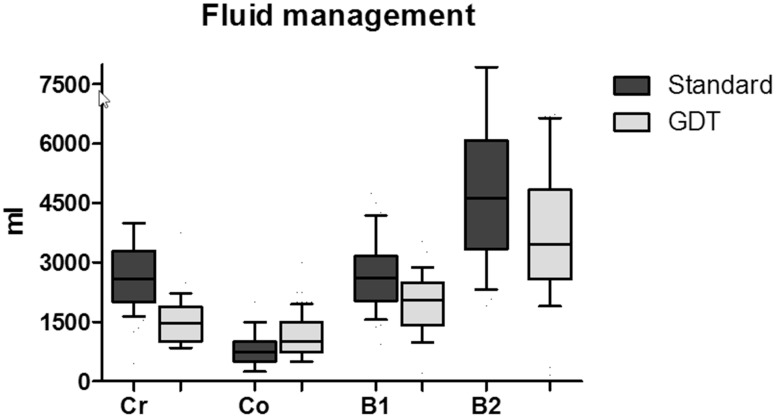
Methods and findings: We compared the postoperative outcome of patients undergoing esophagectomy before (99 patients) and after (100 patients) implementation of GDT. There was no difference in the proportion of patients with a complication (56% vs. 54%, p = 0.82), hospital stay and mortality. The incidence of prolonged ICU stay (>48 hours) was reduced (28% vs. 12, p = .005) in patients treated with GDT. Secondary analysis of complication rate showed a decrease in pneumonia (29 vs. 15%, p = .02), mediastinal abscesses (12 vs. 3%, p = .02), and gastric tube necrosis (5% vs. 0%, p = .03) in patients treated with GDT. Patients in the GDT group received significantly less fluids but received more colloids.
Conclusions: The implementation of GDT during esophagectomy was not associated with reductions in overall morbidity, mortality and hospital length of stay. However, we observed a decrease in pneumonia, mediastinal abscesses, gastric tube necrosis, and ICU length of stay.
Conflict of interest statement
Figures
References
-
- 2015 Clinical audit. http://www.clinicalaudit.nl/jaarrapportage. Accessed April 7, 2015.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
