

Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue: A Meta-analysis
- PMID: 28253393
- PMCID: PMC5557289
- DOI: 10.1001/jamaoncol.2016.6914
Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue: A Meta-analysis
Abstract
Importance: Cancer-related fatigue (CRF) remains one of the most prevalent and troublesome adverse events experienced by patients with cancer during and after therapy.
Objective: To perform a meta-analysis to establish and compare the mean weighted effect sizes (WESs) of the 4 most commonly recommended treatments for CRF-exercise, psychological, combined exercise and psychological, and pharmaceutical-and to identify independent variables associated with treatment effectiveness.
Data sources: PubMed, PsycINFO, CINAHL, EMBASE, and the Cochrane Library were searched from the inception of each database to May 31, 2016.
Study selection: Randomized clinical trials in adults with cancer were selected. Inclusion criteria consisted of CRF severity as an outcome and testing of exercise, psychological, exercise plus psychological, or pharmaceutical interventions.
Data extraction and synthesis: Studies were independently reviewed by 12 raters in 3 groups using a systematic and blinded process for reconciling disagreement. Effect sizes (Cohen d) were calculated and inversely weighted by SE.
Main outcomes and measures: Severity of CRF was the primary outcome. Study quality was assessed using a modified 12-item version of the Physiotherapy Evidence-Based Database scale (range, 0-12, with 12 indicating best quality).
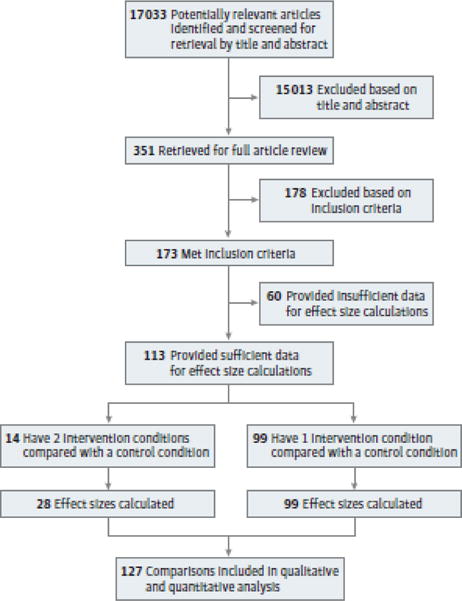
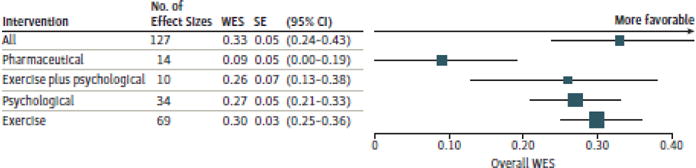
Results: From 17 033 references, 113 unique studies articles (11 525 unique participants; 78% female; mean age, 54 [range, 35-72] years) published from January 1, 1999, through May 31, 2016, had sufficient data. Studies were of good quality (mean Physiotherapy Evidence-Based Database scale score, 8.2; range, 5-12) with no evidence of publication bias. Exercise (WES, 0.30; 95% CI, 0.25-0.36; P < .001), psychological (WES, 0.27; 95% CI, 0.21-0.33; P < .001), and exercise plus psychological interventions (WES, 0.26; 95% CI, 0.13-0.38; P < .001) improved CRF during and after primary treatment, whereas pharmaceutical interventions did not (WES, 0.09; 95% CI, 0.00-0.19; P = .05). Results also suggest that CRF treatment effectiveness was associated with cancer stage, baseline treatment status, experimental treatment format, experimental treatment delivery mode, psychological mode, type of control condition, use of intention-to-treat analysis, and fatigue measures (WES range, -0.91 to 0.99). Results suggest that the effectiveness of behavioral interventions, specifically exercise and psychological interventions, is not attributable to time, attention, and education, and specific intervention modes may be more effective for treating CRF at different points in the cancer treatment trajectory (WES range, 0.09-0.22).
Conclusions and relevance: Exercise and psychological interventions are effective for reducing CRF during and after cancer treatment, and they are significantly better than the available pharmaceutical options. Clinicians should prescribe exercise or psychological interventions as first-line treatments for CRF.
Conflict of interest statement
Figures
Comment in
-
Exercise and Psychological Interventions are Best for Cancer-Related Fatigue.Am J Nurs. 2017 Jul;117(7):63. doi: 10.1097/01.NAJ.0000520950.69718.38. Am J Nurs. 2017. PMID: 28644294 No abstract available.
-
Difficulties in Defining and Measuring Cancer-Related Fatigue.JAMA Oncol. 2018 Mar 1;4(3):418-419. doi: 10.1001/jamaoncol.2017.3355. JAMA Oncol. 2018. PMID: 28983559 No abstract available.
-
Difficulties in Defining and Measuring Cancer-Related Fatigue-Reply.JAMA Oncol. 2018 Mar 1;4(3):419-420. doi: 10.1001/jamaoncol.2017.3358. JAMA Oncol. 2018. PMID: 28983561 No abstract available.
References
-
- Patrick DL, Ferketich SL, Frame PS, et al. National Institutes of Health State-of-the-Science Panel National Institutes of Health State-of-the-Science Conference Statement: symptom management in cancer: pain, depression, and fatigue, July 15–17, 2002. J Natl Cancer Inst. 2003;95(15):1110–1117. - PubMed
-
- Henry DH, Viswanathan HN, Elkin EP, Traina S, Wade S, Cella D. Symptoms and treatment burden associated with cancer treatment. Support Care Cancer. 2008;16(7):791–801. - PubMed
-
- Kuhnt S, Ernst J, Singer S, et al. Fatigue in cancer survivors—prevalence and correlates. Onkologie. 2009;32(6):312–31. - PubMed
-
- Servaes P, Verhagen C, Bleijenberg G. Fatigue in cancer patients during and after treatment: prevalence, correlates and interventions. Eur J Cancer. 2002;38(1):27–43. - PubMed
-
- Lawrence DP, Kupelnick B, Miller K, Devine D, Lau J. Evidence report on the occurrence, assessment, and treatment of fatigue in cancer patients. J Natl Cancer Inst Monogr. 2004;(32):40–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
