

Counting the lives saved by DOTS in India: a model-based approach
- PMID: 28253922
- PMCID: PMC5335816
- DOI: 10.1186/s12916-017-0809-5
Counting the lives saved by DOTS in India: a model-based approach
Abstract
Background: Against the backdrop of renewed efforts to control tuberculosis (TB) worldwide, there is a need for improved methods to estimate the public health impact of TB programmes. Such methods should not only address the improved outcomes amongst those receiving care but should also account for the impact of TB services on reducing transmission.
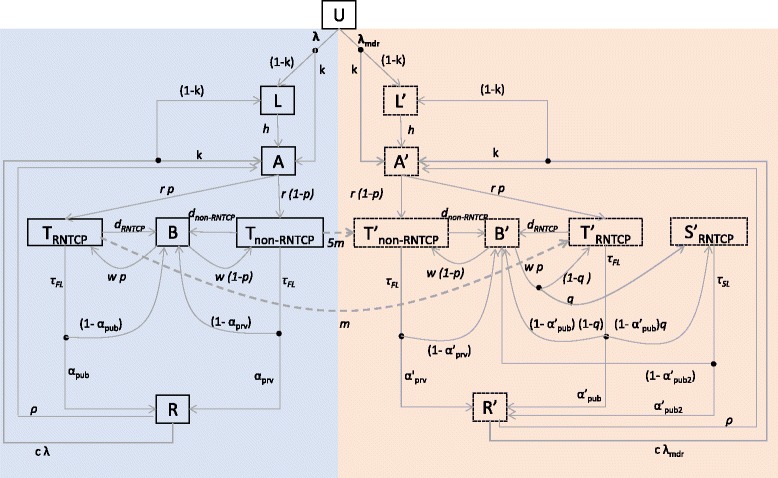
Methods: Vital registration data in India are not sufficiently reliable for estimates of TB mortality. As an alternative approach, we developed a mathematical model of TB transmission dynamics and mortality, capturing the scale-up of DOTS in India, through the rollout of the Revised National TB Control Programme (RNTCP). We used available data from the literature to calculate TB mortality hazards amongst untreated TB; amongst cases treated under RNTCP; and amongst cases treated under non-RNTCP conditions. Using a Bayesian evidence synthesis framework, we combined these data with current estimates for the TB burden in India to calibrate the transmission model. We simulated the national TB epidemic in the presence and absence of the DOTS programme, measuring lives saved as the difference in TB deaths between these scenarios.
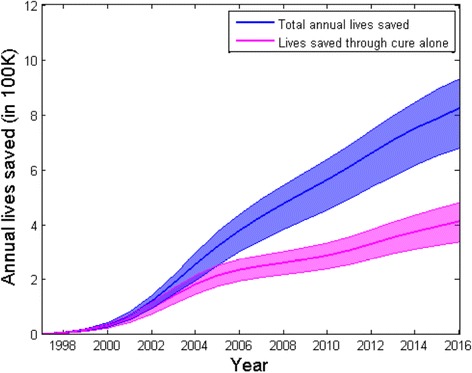
Results: From 1997 to 2016, India's RNTCP has saved 7.75 million lives (95% Bayesian credible interval 6.29-8.82 million). We estimate that 42% of this impact was due to the 'indirect' effects of the RNTCP in averting transmission as well as improving treatment outcomes.
Conclusions: When expanding high-quality TB services, a substantial proportion of overall impact derives from preventive, as well as curative, benefits. Mathematical models, together with sufficient data, can be a helpful tool in estimating the true population impact of major disease control programmes.
Keywords: Deaths averted; India; Modelling; Tuberculosis.
Figures


References
-
- World Health Organization. Global tuberculosis report 2016. World Health Organization 2016. WHO Press, Geneva. WHO/HTM/TB/2016.13.
-
- World Health Organization.A brief history of tuberculosis control in India. 2010. http://apps.who.int/iris/bitstream/10665/44408/1/9789241500159_eng.pdf. Accessed 02 Jan 2017.
-
- World Health Organization. Millennium Development Goals (MDGs) MDG 6: combat HIV/AIDS, malaria and other diseases. 2014. http://www.who.int/topics/millennium_development_goals/diseases/en/. Accessed 13 Sept 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
