Telomere-driven diseases and telomere-targeting therapies
- PMID: 28254828
- PMCID: PMC5379954
- DOI: 10.1083/jcb.201610111
Telomere-driven diseases and telomere-targeting therapies
Abstract
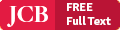
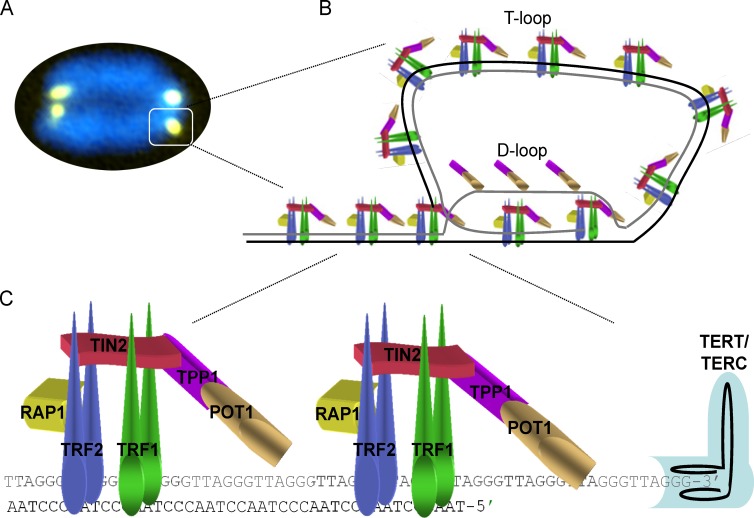
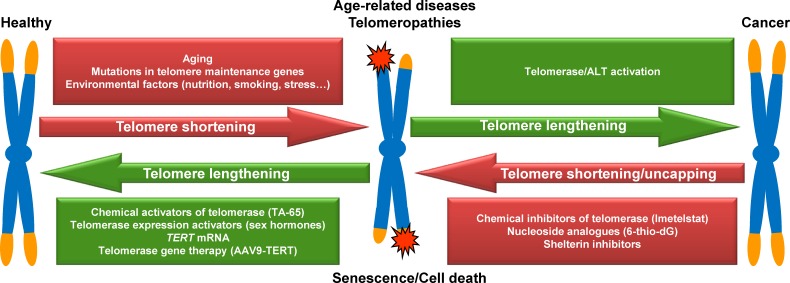
Telomeres, the protective ends of linear chromosomes, shorten throughout an individual's lifetime. Telomere shortening is proposed to be a primary molecular cause of aging. Short telomeres block the proliferative capacity of stem cells, affecting their potential to regenerate tissues, and trigger the development of age-associated diseases. Mutations in telomere maintenance genes are associated with pathologies referred to as telomere syndromes, including Hoyeraal-Hreidarsson syndrome, dyskeratosis congenita, pulmonary fibrosis, aplastic anemia, and liver fibrosis. Telomere shortening induces chromosomal instability that, in the absence of functional tumor suppressor genes, can contribute to tumorigenesis. In addition, mutations in telomere length maintenance genes and in shelterin components, the protein complex that protects telomeres, have been found to be associated with different types of cancer. These observations have encouraged the development of therapeutic strategies to treat and prevent telomere-associated diseases, namely aging-related diseases, including cancer. Here we review the molecular mechanisms underlying telomere-driven diseases and highlight recent advances in the preclinical development of telomere-targeted therapies using mouse models.
© 2017 Martínez and Blasco.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources