

Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients
- PMID: 28255002
- PMCID: PMC5461792
- DOI: 10.1681/ASN.2016070797
Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients
Abstract
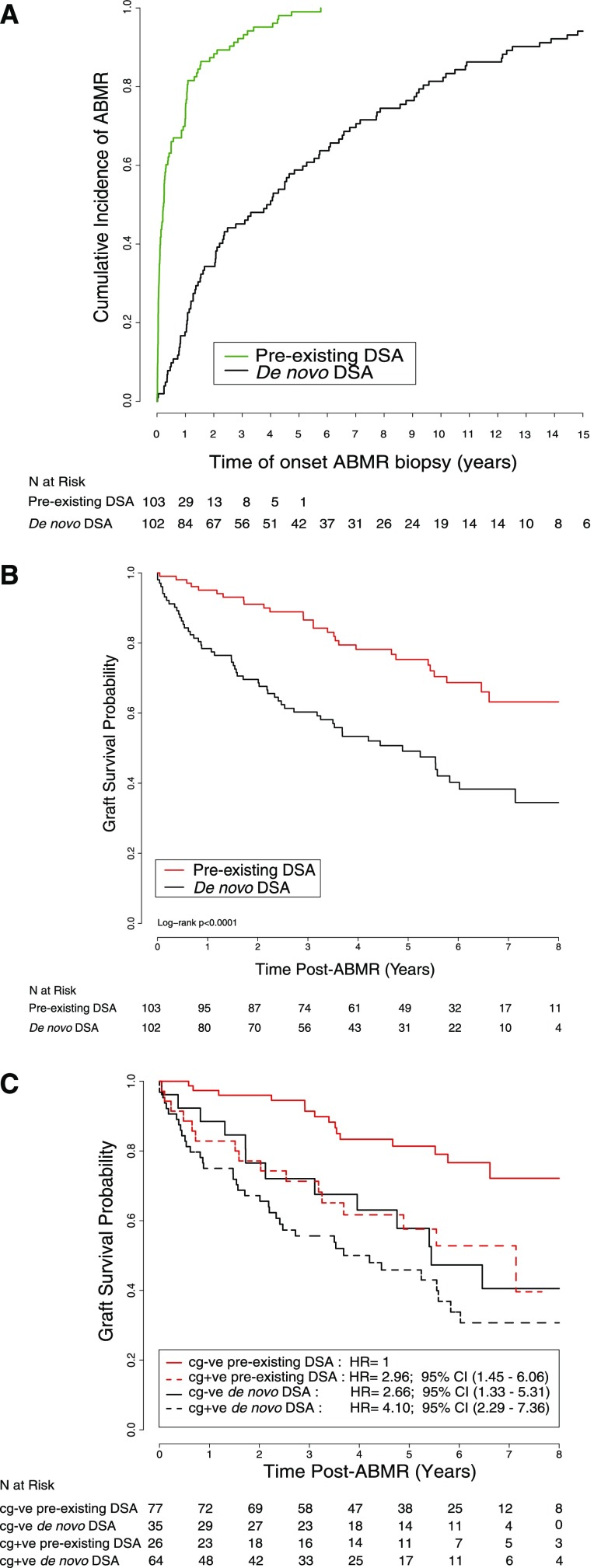
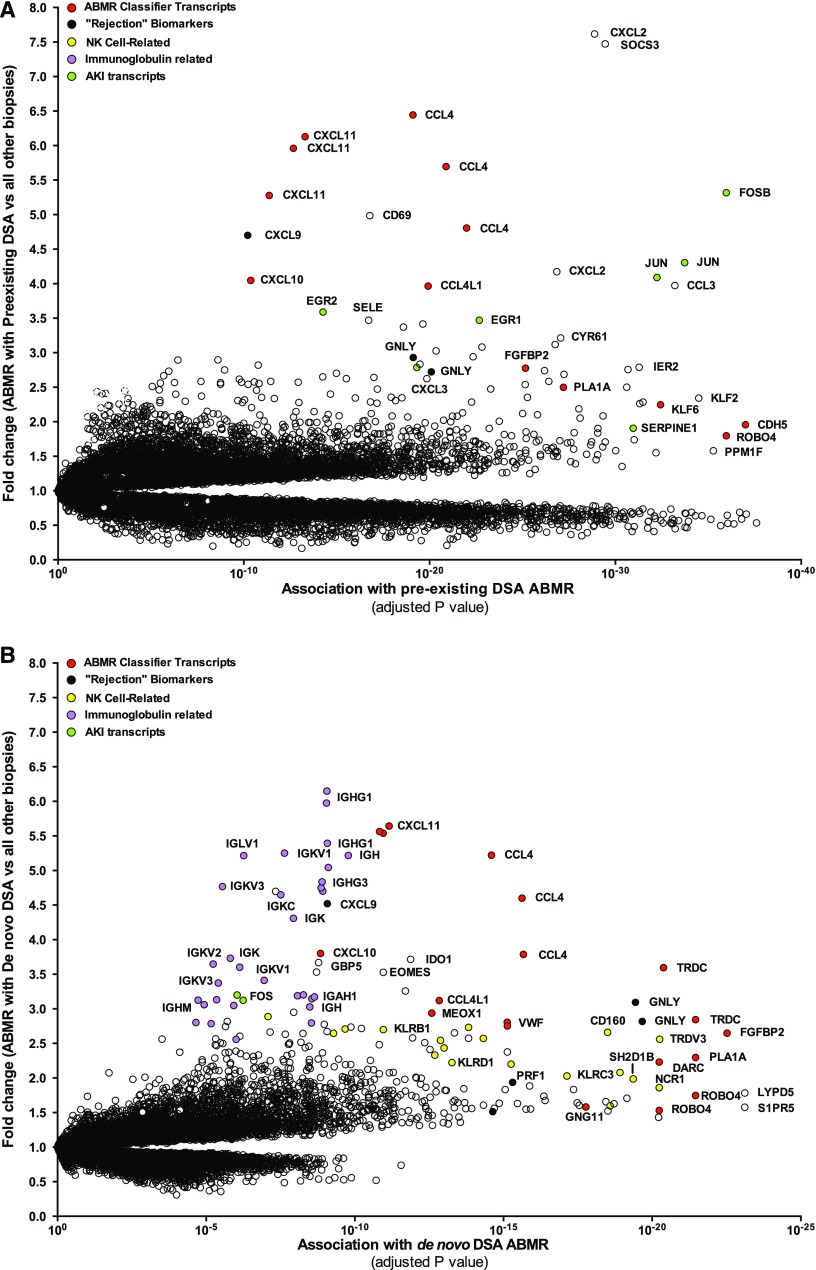
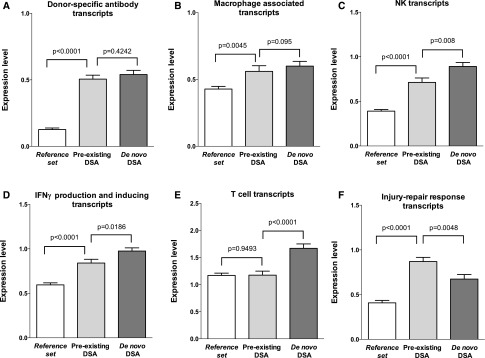
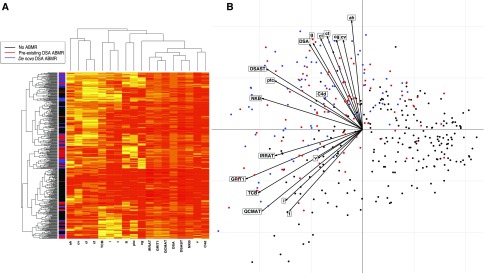
Antibody-mediated rejection (ABMR) can occur in patients with preexisting anti-HLA donor-specific antibodies (DSA) or in patients who develop de novo DSA. However, how these processes compare in terms of allograft injury and outcome has not been addressed. From a cohort of 771 kidney biopsy specimens from two North American and five European centers, we performed a systematic assessment of clinical and biologic parameters, histopathology, circulating DSA, and allograft gene expression for all patients with ABMR (n=205). Overall, 103 (50%) patients had preexisting DSA and 102 (50%) had de novo DSA. Compared with patients with preexisting DSA ABMR, patients with de novo DSA ABMR displayed increased proteinuria, more transplant glomerulopathy lesions, and lower glomerulitis, but similar levels of peritubular capillaritis and C4d deposition. De novo DSA ABMR was characterized by increased expression of IFNγ-inducible, natural killer cell, and T cell transcripts, but less expression of AKI transcripts compared with preexisting DSA ABMR. The preexisting DSA ABMR had superior graft survival compared with the de novo DSA ABMR (63% versus 34% at 8 years after rejection, respectively; P<0.001). After adjusting for clinical, histologic, and immunologic characteristics and treatment, we identified de novo DSA ABMR (hazard ratio [HR], 1.82 compared with preexisting DSA ABMR; 95% confidence interval [95% CI], 1.07 to 3.08; P=0.03); low eGFR (<30 ml/min per 1.73 m2) at diagnosis (HR, 3.27; 95% CI, 1.48 to 7.23; P<0.001); ≥0.30 g/g urine protein-to-creatinine ratio (HR, 2.44; 95% CI, 1.47 to 4.09; P<0.001); and presence of cg lesions (HR, 2.25; 95% CI, 1.34 to 3.79; P=0.002) as the main independent determinants of allograft loss. Our findings support the transplant of kidneys into highly sensitized patients and should encourage efforts to monitor patients for de novo DSA.
Keywords: antibody-mediated rejection; donor-specific anti-HLA antibody; kidney transplantation; microscope; molecular; transplant outcomes.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Nankivell BJ, Alexander SI: Rejection of the kidney allograft. N Engl J Med 363: 1451–1462, 2010 - PubMed
-
- Sellarés J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF: Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12: 388–399, 2012 - PubMed
-
- Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, Kaplan B, Halloran PF: Antibody-mediated microcirculation injury is the major cause of late kidney transplant failure. Am J Transplant 9: 2520–2531, 2009 - PubMed
-
- Aubert O, Kamar N, Vernerey D, Viglietti D, Martinez F, Duong-Van-Huyen JP, Eladari D, Empana JP, Rabant M, Verine J, Rostaing L, Congy N, Guilbeau-Frugier C, Mourad G, Garrigue V, Morelon E, Giral M, Kessler M, Ladrière M, Delahousse M, Glotz D, Legendre C, Jouven X, Lefaucheur C, Loupy A: Long term outcomes of transplantation using kidneys from expanded criteria donors: Prospective, population based cohort study. BMJ 351: h3557, 2015 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
