

Clinical and Imaging Characteristics of Diffuse Intracranial Dolichoectasia
- PMID: 28255032
- PMCID: PMC7960370
- DOI: 10.3174/ajnr.A5102
Clinical and Imaging Characteristics of Diffuse Intracranial Dolichoectasia
Abstract
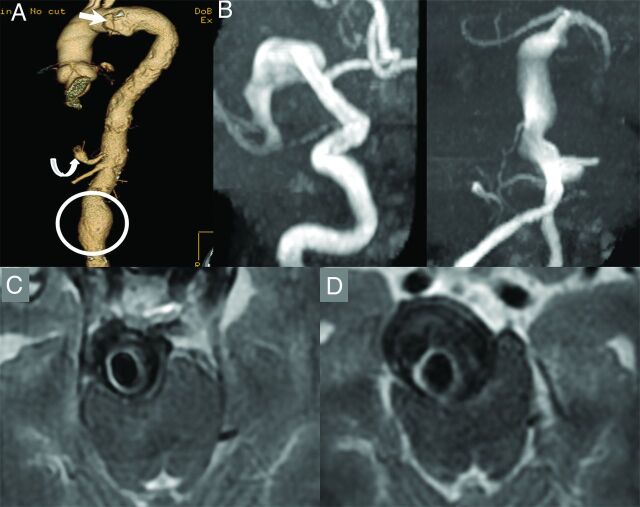
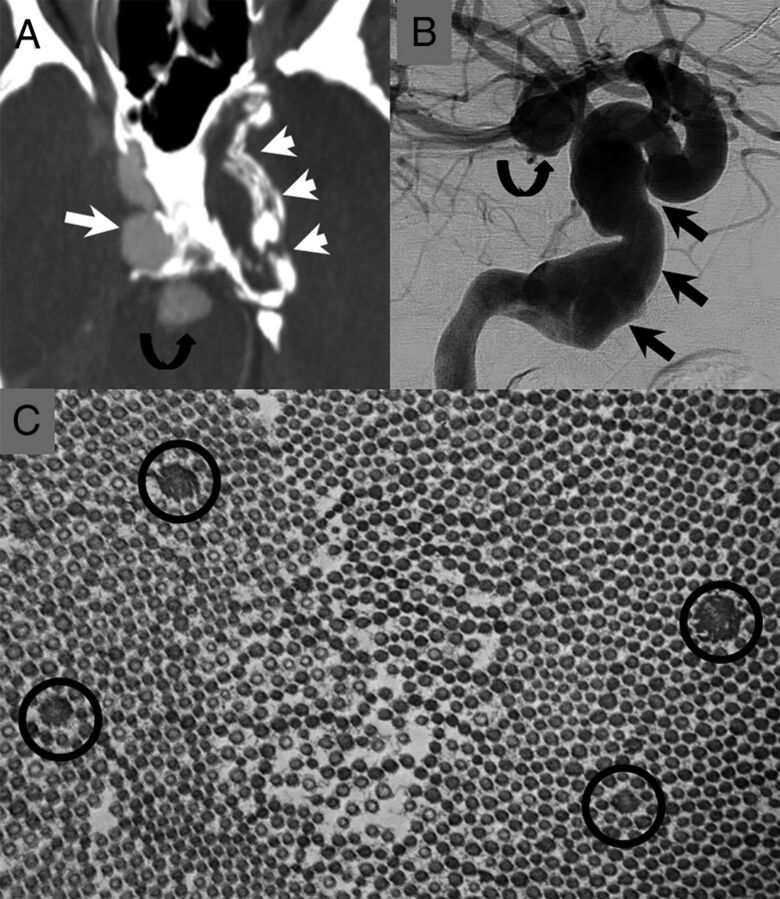
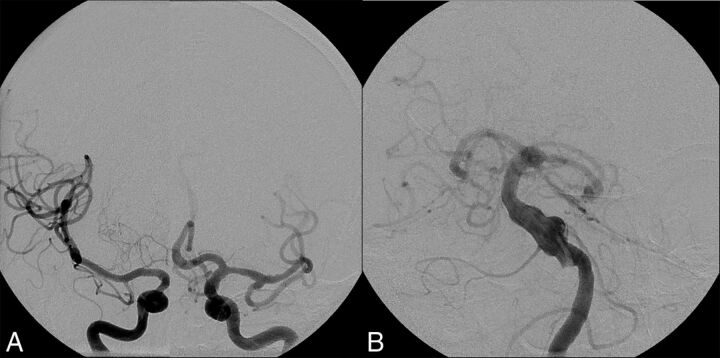
Background and purpose: Among patients with vertebrobasilar dolichoectasia is a subset of patients with disease affecting the anterior circulation as well. We hypothesized that multivessel intracranial dolichoectasia may represent a distinct phenotype from single-territory vertebrobasilar dolichoectasia. The purpose of this study was to characterize clinical characteristics and angiographic features of this proposed distinct phenotype termed "diffuse intracranial dolichoectasia" and compare them with those in patients with isolated vertebrobasilar dolichoectasia.
Materials and methods: We retrospectively reviewed a consecutive series of patients with diffuse intracranial dolichoectasia and compared their demographics, vascular risk factors, additional aneurysm prevalence, and clinical outcomes with a group of patients with vertebrobasilar dolichoectasia. "Diffuse intracranial dolichoectasia" was defined as aneurysmal dilation of entire vascular segments involving ≥2 intracranial vascular beds. Categoric and continuous variables were compared by using χ2 and Student t tests, respectively.
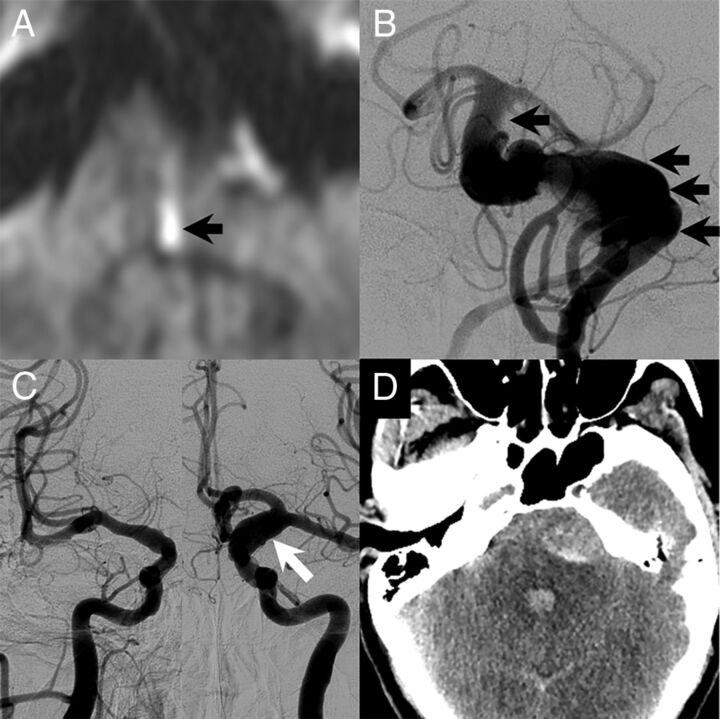
Results: Twenty-five patients had diffuse intracranial dolichoectasia, and 139 had vertebrobasilar dolichoectasia. Patients with diffuse intracranial dolichoectasia were older than those with vertebrobasilar dolichoectasia (70.9 ± 14.2 years versus 60.4 ± 12.5 years, P = .0002) and had a higher prevalence of abdominal aortic aneurysms (62.5% versus 14.3%, P = .01), other visceral aneurysms (25.0% versus 0%, P < .0001), and smoking (68.0% versus 15.9%, P < .0001). Patients with diffuse intracranial dolichoectasia were more likely to have aneurysm growth (46.2% versus 21.5%, P = .09) and rupture (20% versus 3.5%, P = .007) at follow-up. Patients with diffuse intracranial dolichoectasia were less likely to have good neurologic function at follow-up (24.0% versus 57.6%, P = .004) and were more likely to have aneurysm-related death (24.0% versus 7.2%, P = .02).
Conclusions: The natural history of patients with diffuse intracranial dolichoectasia is significantly worse than that in those with isolated vertebrobasilar dolichoectasia. Many patients with diffuse intracranial dolichoectasia had additional saccular and abdominal aortic aneurysms. These findings suggest that diffuse intracranial dolichoectasia may be a distinct vascular phenotype secondary to a systemic arteriopathy affecting multiple vascular beds.
© 2017 by American Journal of Neuroradiology.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical