

Echocardiographic Screening for Rheumatic Heart Disease in Indigenous Australian Children: A Cost-Utility Analysis
- PMID: 28255077
- PMCID: PMC5524001
- DOI: 10.1161/JAHA.116.004515
Echocardiographic Screening for Rheumatic Heart Disease in Indigenous Australian Children: A Cost-Utility Analysis
Abstract
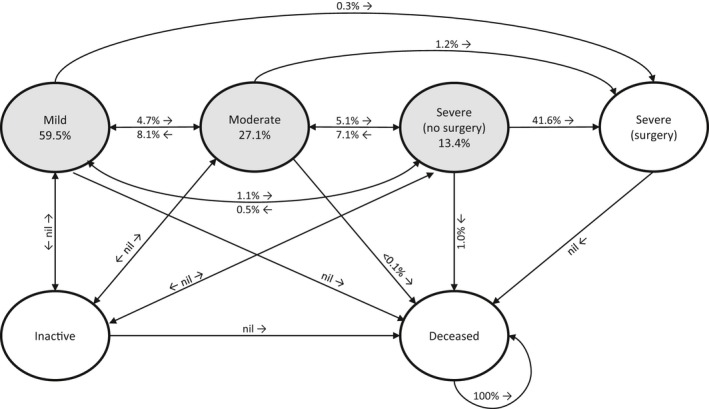
Background: Rheumatic heart disease (RHD) remains a leading cause of cardiovascular morbidity and mortality in children and young adults in disadvantaged populations. The emergence of echocardiographic screening provides the opportunity for early disease detection and intervention. Using our own multistate model of RHD progression derived from Australian RHD register data, we performed a cost-utility analysis of echocardiographic screening in indigenous Australian children, with the dual aims of informing policy decisions in Australia and providing a model that could be adapted in other countries.
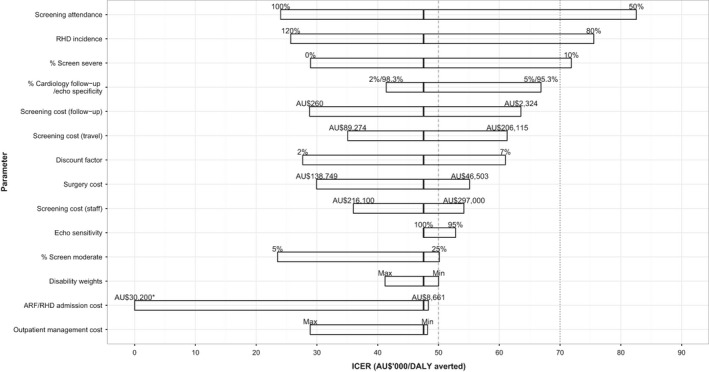
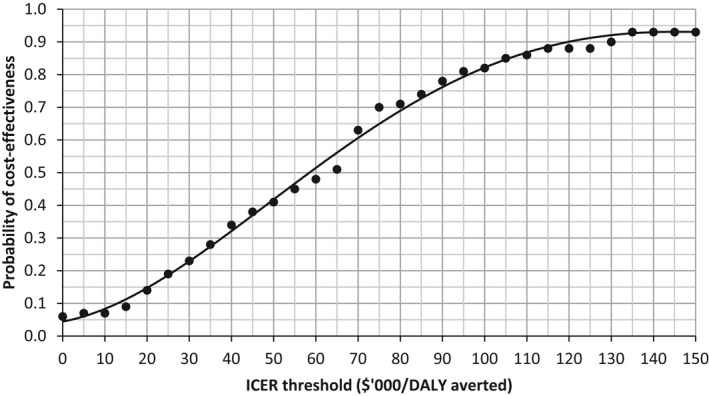
Methods and results: We simulated the outcomes of 2 screening strategies, assuming that RHD could be detected 1, 2, or 3 years earlier by screening. Outcomes included reductions in heart failure, surgery, mortality, disability-adjusted life-years, and corresponding costs. Only a strategy of screening all indigenous 5- to 12-year-olds in half of their communities in alternate years was found to be cost-effective (incremental cost-effectiveness ratio less than AU$50 000 per disability-adjusted life-year averted), assuming that RHD can be detected at least 2 years earlier by screening; however, this result was sensitive to a number of assumptions. Additional modeling of improved adherence to secondary prophylaxis alone resulted in dramatic reductions in heart failure, surgery, and death; these outcomes improved even further when combined with screening.
Conclusions: Echocardiographic screening for RHD is cost-effective in our context, assuming that RHD can be detected ≥2 years earlier by screening. Our model can be adapted to any other setting but will require local data or acceptable assumptions for model parameters.
Keywords: cost‐effectiveness; echocardiography; pediatrics; rheumatic heart disease; screening.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Comment in
-
Clinical Impact and Costs of Echocardiographic Screening for Rheumatic Heart Disease.J Am Heart Assoc. 2017 Mar 2;6(3):e005666. doi: 10.1161/JAHA.117.005666. J Am Heart Assoc. 2017. PMID: 28255081 Free PMC article. No abstract available.
References
-
- World Health Organization . WHO Technical Report Series; 923. Rheumatic fever and rheumatic heart disease. Report of a WHO Expert Consultation, Geneva, 29 October–1 November 2001. Geneva; 2004. - PubMed
-
- Saxena A, Zuhlke L, Wilson N. Echocardiographic screening for rheumatic heart disease: issues for the cardiology community. Glob Heart. 2013;8:197–202. - PubMed
-
- Zuhlke L, Mayosi BM. Echocardiographic screening for subclinical rheumatic heart disease remains a research tool pending studies of impact on prognosis. Curr Cardiol Rep. 2013;15:343. - PubMed
-
- Roberts K, Colquhoun S, Steer A, Remenyi B, Carapetis J. Screening for rheumatic heart disease: current approaches and controversies. Nat Rev Cardiol. 2013;10:49–58. - PubMed
-
- Remenyi B, Wilson N, Steer A, Ferreira B, Kado J, Kumar K, Lawrenson J, Maguire G, Marijon E, Mirabel M, Mocumbi AO, Mota C, Paar J, Saxena A, Scheel J, Stirling J, Viali S, Balekundri VI, Wheaton G, Zuhlke L, Carapetis J. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease‐an evidence‐based guideline. Nat Rev Cardiol. 2012;9:297–309. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
