

Natural course of early COPD
- PMID: 28255237
- PMCID: PMC5325091
- DOI: 10.2147/COPD.S122989
Natural course of early COPD
Abstract
Background and objective: Few studies have examined the natural course of early COPD. The aim of this study was to observe the natural course of early COPD patients. We also aimed to analyze medical utilization and costs for early COPD during a 6-year period.
Methods: Patients with early COPD were selected from Korean National Health and Nutrition Examination Survey (KNHANES) data. We linked the KNHANES data of patients with early COPD to National Health Insurance data.
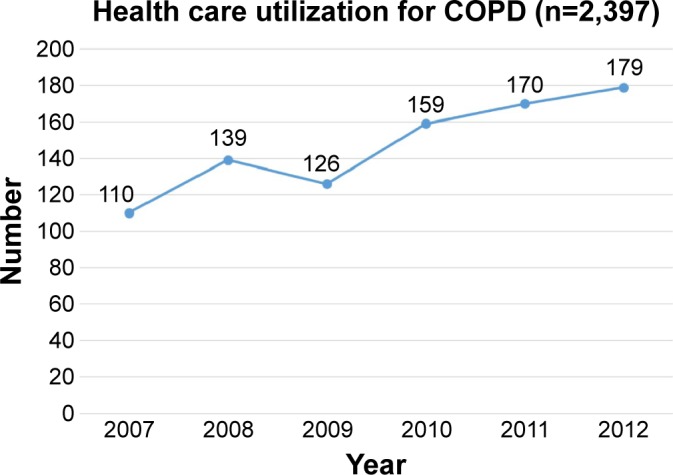
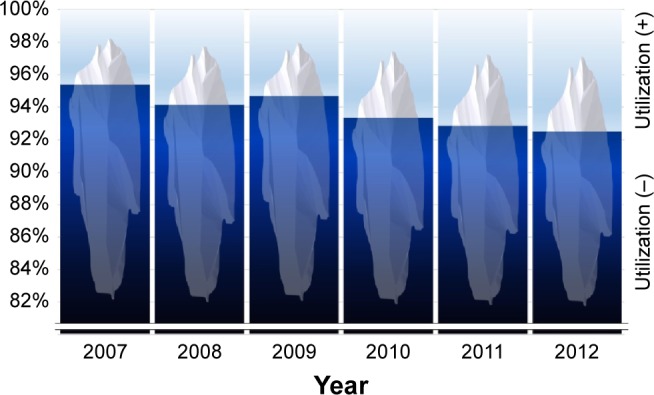
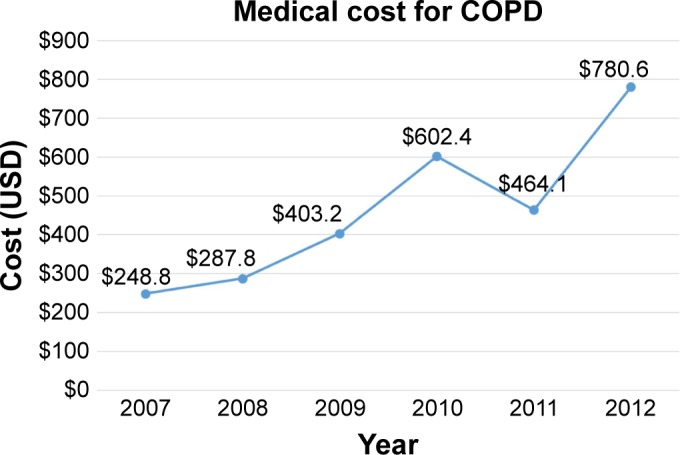
Results: A total of 2,397 patients were enrolled between 2007 and 2012. The mean forced expiratory volume in 1 second (FEV1) was 78.6%, and the EuroQol five dimensions questionnaire (EQ-5D) index value was 0.9. In total, 110 patients utilized health care for COPD in 2007, and this number increased to 179 in 2012. The total mean number of days used per person increased from 4.9 in 2007 to 7.8 in 2012. The total medical cost per person also increased from 248.8 US dollar (USD) in 2007 to 780.6 USD in 2013. A multiple linear regression revealed that age, lower body mass index, lower FEV1 (%), and lower EQ-5D score were significantly associated with medical costs.
Conclusion: Even in early COPD patients, some of them eventually progressed and utilized health care for COPD.
Keywords: HIRA; KNHANES; NHI; cost; early COPD; utilization.
Conflict of interest statement
Disclosure CKR received consulting/lecture fees from MSD, AstraZeneca, Novartis, GSK, Takeda, Mundipharma, Sandoz, Boehringer-Ingelheim, and Teva-Handok. The other authors report no conflicts of interest in this work.
Figures
References
-
- Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2016. [Accessed October 15, 2016]. Available from: http://goldcopd.org/global-strategy-diagnosis-management-prevention-copd...
-
- Antonelli-Incalzi R, Imperiale C, Bellia V, et al. SaRA Investigators Do GOLD stages of COPD severity really correspond to differences in health status? Eur Respir J. 2003;22(3):444–449. - PubMed
-
- Guirguis-Blake JM, Senger CA, Webber EM, Mularski RA, Whitlock EP. Screening for chronic obstructive pulmonary disease: evidence report and systematic review for the US preventive services task force. JAMA. 2016;315(13):1378–1393. - PubMed
-
- Decramer M, Cooper CB. Treatment of COPD: the sooner the better? Thorax. 2010;65(9):837–841. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
