

Prognostic significance of tumor budding and single cell invasion in gastric adenocarcinoma
- PMID: 28255247
- PMCID: PMC5325090
- DOI: 10.2147/OTT.S127762
Prognostic significance of tumor budding and single cell invasion in gastric adenocarcinoma
Abstract
Purpose: Gastric carcinoma (GC) is a highly aggressive cancer and one of the leading causes of cancer-related deaths worldwide. Histopathological evaluation pertaining to invasiveness is likely to provide additional information in relation to patient outcome. In this study, we aimed to evaluate the prognostic significance of tumor budding and single cell invasion in gastric adenocarcinoma.
Materials and methods: Hematoxylin and eosin-stained slides generated from 296 gastric adenocarcinoma patients with full clinical and pathological and follow-up information were systematically reviewed. The patients were grouped on the basis of tumor budding, single cell invasion, large cell invasion, mitotic count, and fibrosis. The association between histopathological parameters, different classification systems, and overall survival (OS) was statistically analyzed.
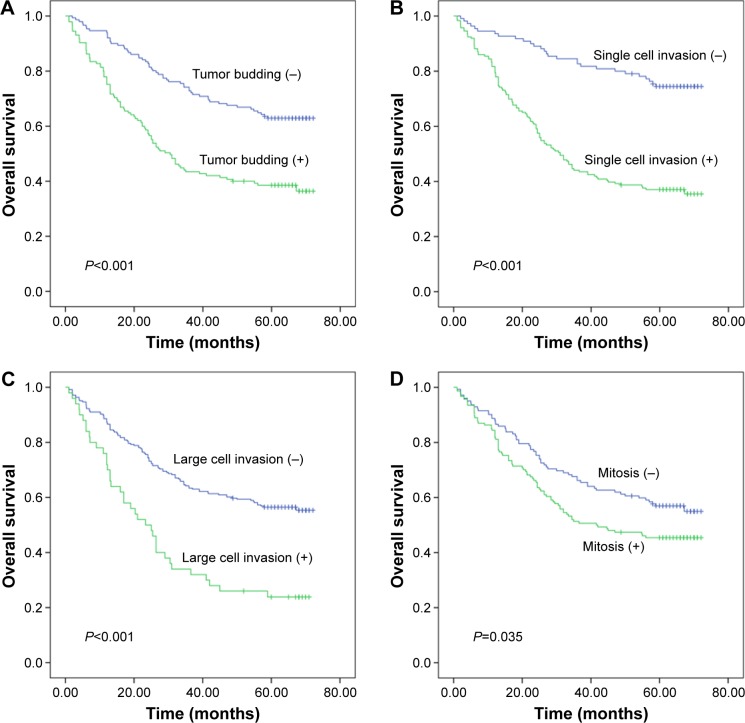
Results: Among the 296 cases that were analyzed, high-grade tumor budding was observed in 49.0% (145) of them. Single cell invasion and large cell invasion were observed in 62.8% (186) and 16.9% (50) of the cases, respectively. Following univariate analysis, patients with high-grade tumor budding had shorter OS than those with low-grade tumor budding (hazard ratio [HR]: 2.260, P<0.001). Similarly, the OS of patients with single cell invasion and large cell invasion was reduced (single cell invasion, HR: 3.553, P<0.001; large cell invasion, HR: 2.466, P<0.001). Following multivariate analysis, tumor budding and single cell invasion were observed to be independent risk factors for gastric adenocarcinoma (P<0.05). According to the Lauren classification, patients with intestinal-type adenocarcinoma had better outcomes than those with diffuse-type adenocarcinoma (HR: 2.563, P<0.001).
Conclusion: Tumor budding and single cell invasion in gastric adenocarcinoma are associated with an unfavorable prognosis.
Keywords: gastric carcinoma; invasion type; metastasis; pathology; prognosis.
Conflict of interest statement
Disclosure All authors report no conflicts of interest in this work.
Figures


Similar articles
-
Tumor budding as a prognostic factor in pancreatic ductal adenocarcinoma.Virchows Arch. 2020 Apr;476(4):561-568. doi: 10.1007/s00428-019-02719-1. Epub 2019 Nov 30. Virchows Arch. 2020. PMID: 31786688
-
Prognostic and pathological impact of tumor budding in gastric cancer: A systematic review and meta-analysis.World J Gastrointest Oncol. 2019 Oct 15;11(10):898-908. doi: 10.4251/wjgo.v11.i10.898. World J Gastrointest Oncol. 2019. PMID: 31662828 Free PMC article.
-
Prognostic Impact of Tumor Budding on Moroccan Gastric Cancer Patients.Clin Pathol. 2023 Jun 27;16:2632010X231184329. doi: 10.1177/2632010X231184329. eCollection 2023 Jan-Dec. Clin Pathol. 2023. PMID: 37426068 Free PMC article.
-
Tumor budding is a prognostic factor linked to epithelial mesenchymal transition in pancreatic ductal adenocarcinoma. Study report and literature review.Pancreatology. 2018 Jan;18(1):79-84. doi: 10.1016/j.pan.2017.11.010. Epub 2017 Nov 21. Pancreatology. 2018. PMID: 29233500 Review.
-
Tumor budding in upper gastrointestinal carcinomas.Front Oncol. 2014 Aug 14;4:216. doi: 10.3389/fonc.2014.00216. eCollection 2014. Front Oncol. 2014. PMID: 25177546 Free PMC article. Review.
Cited by
-
Tumor Budding Detection System in Whole Slide Pathology Images.J Med Syst. 2019 Dec 18;44(2):38. doi: 10.1007/s10916-019-1515-y. J Med Syst. 2019. PMID: 31853654
-
Prognostic role of tumor budding in breast cancer.World J Exp Med. 2018 Sep 7;8(2):12-17. doi: 10.5493/wjem.v8.i2.12. eCollection 2018 Sep 7. World J Exp Med. 2018. PMID: 30211020 Free PMC article.
-
Potential key roles of tumour budding: a representative malignant pathological feature of non-small cell lung cancer and a sensitive indicator of prognosis.BMJ Open. 2022 Mar 31;12(3):e054009. doi: 10.1136/bmjopen-2021-054009. BMJ Open. 2022. PMID: 35361643 Free PMC article.
-
Three-dimensional analysis of extrahepatic cholangiocarcinoma and tumor budding.J Pathol. 2020 Aug;251(4):400-410. doi: 10.1002/path.5474. Epub 2020 Jul 3. J Pathol. 2020. PMID: 32476131 Free PMC article.
-
Tumor budding as an indicator for lymph node metastasis and prognosis of early gastric cancer.J Cancer Res Clin Oncol. 2023 Aug;149(9):5603-5616. doi: 10.1007/s00432-022-04522-z. Epub 2022 Dec 13. J Cancer Res Clin Oncol. 2023. PMID: 36512103 Free PMC article.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. - PubMed
-
- Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345(10):725–730. - PubMed
-
- Glynne-Jones R, Nilsson PJ, Aschele C, et al. Anal cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Radiother Oncol. 2014;111(3):330–339. - PubMed
-
- Ajani JA, Eisenberg B, Emanuel P, et al. NCCN practice guidelines for upper gastrointestinal carcinomas. Oncology. 1998;12(11 A):179–223. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
