

Development of a Patient-Specific Finite Element Model for Predicting Implant Failure in Pelvic Ring Fracture Fixation
- PMID: 28255332
- PMCID: PMC5309420
- DOI: 10.1155/2017/9403821
Development of a Patient-Specific Finite Element Model for Predicting Implant Failure in Pelvic Ring Fracture Fixation
Erratum in
-
Corrigendum to "Development of a Patient-Specific Finite Element Model for Predicting Implant Failure in Pelvic Ring Fracture Fixation".Comput Math Methods Med. 2017;2017:8956549. doi: 10.1155/2017/8956549. Epub 2017 Nov 23. Comput Math Methods Med. 2017. PMID: 29333195 Free PMC article.
Abstract
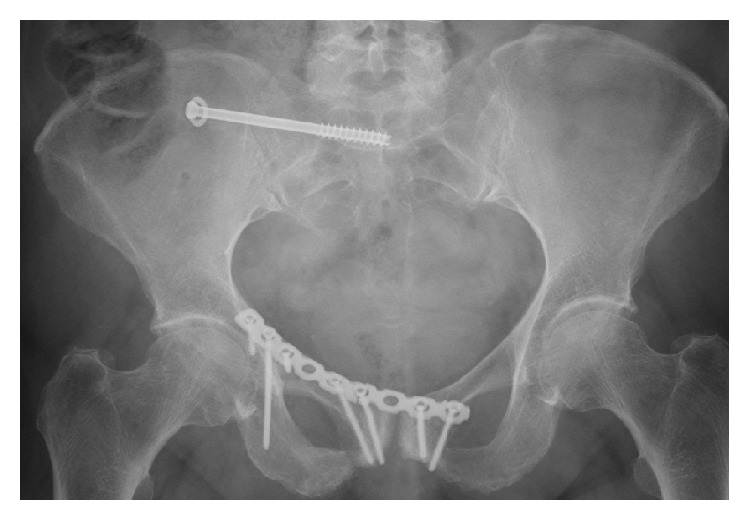
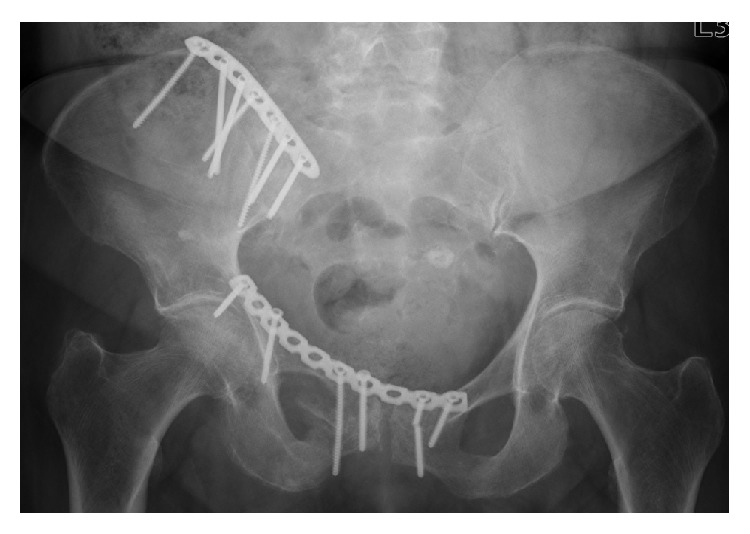
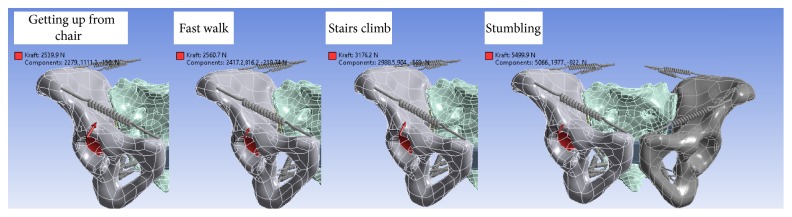
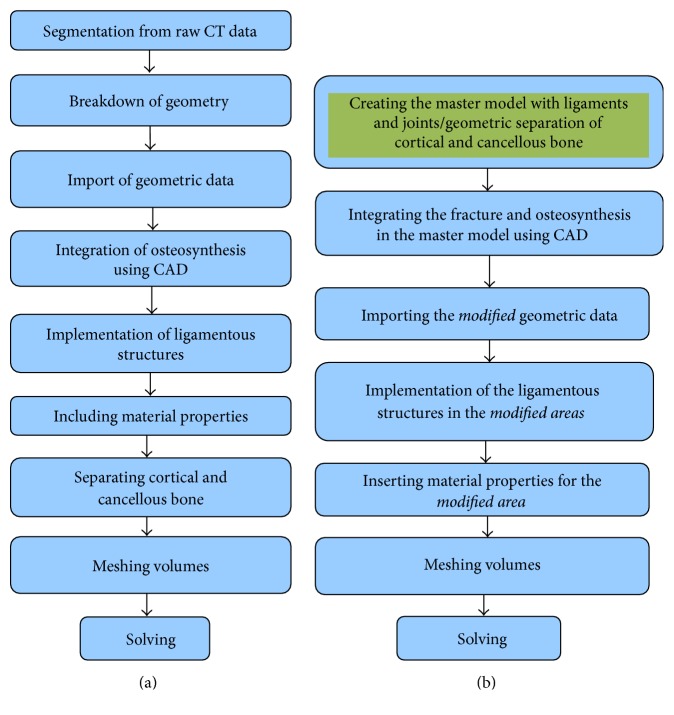
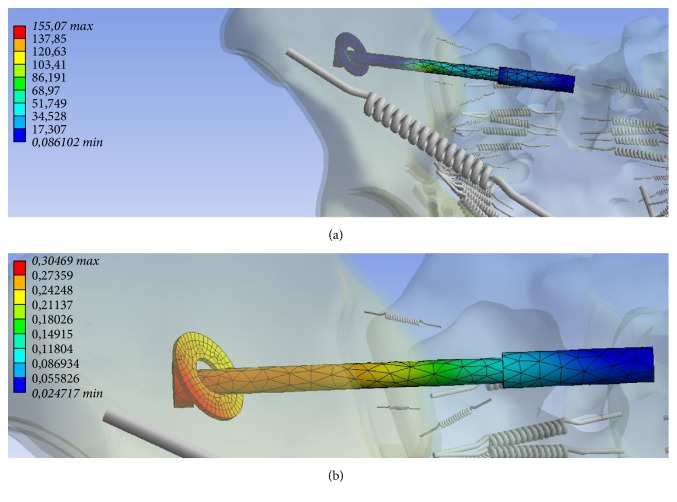
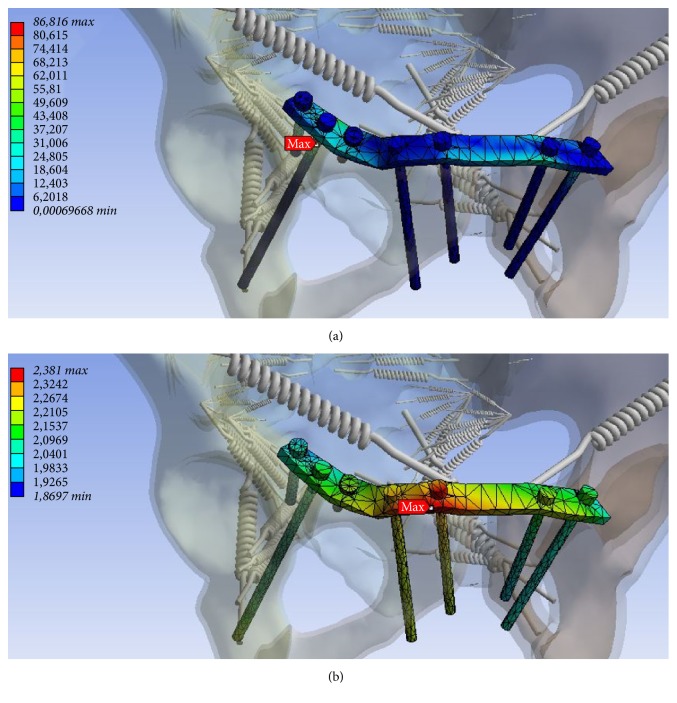
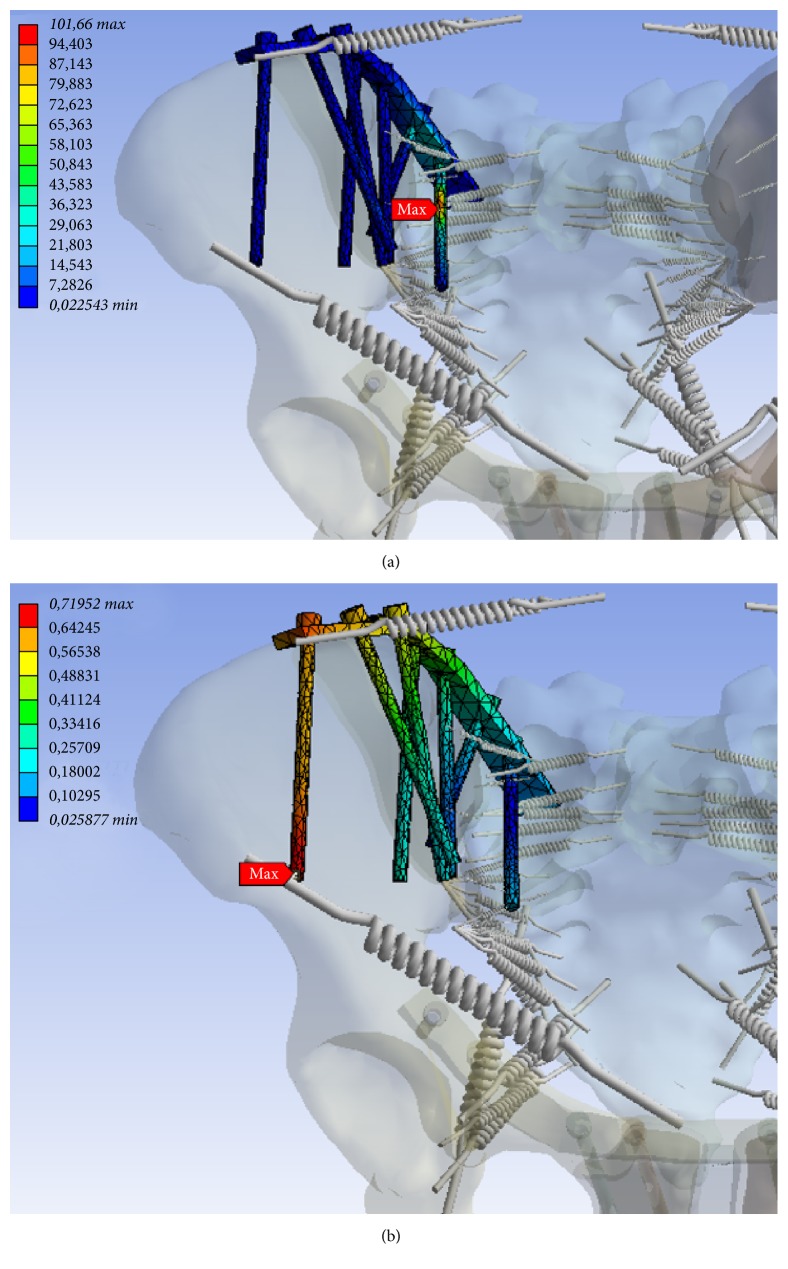
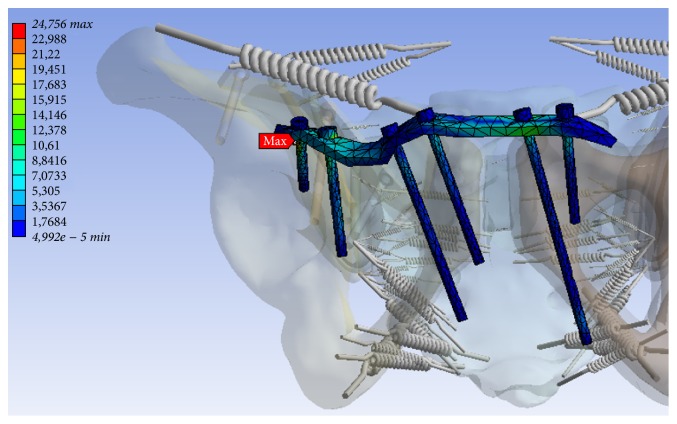
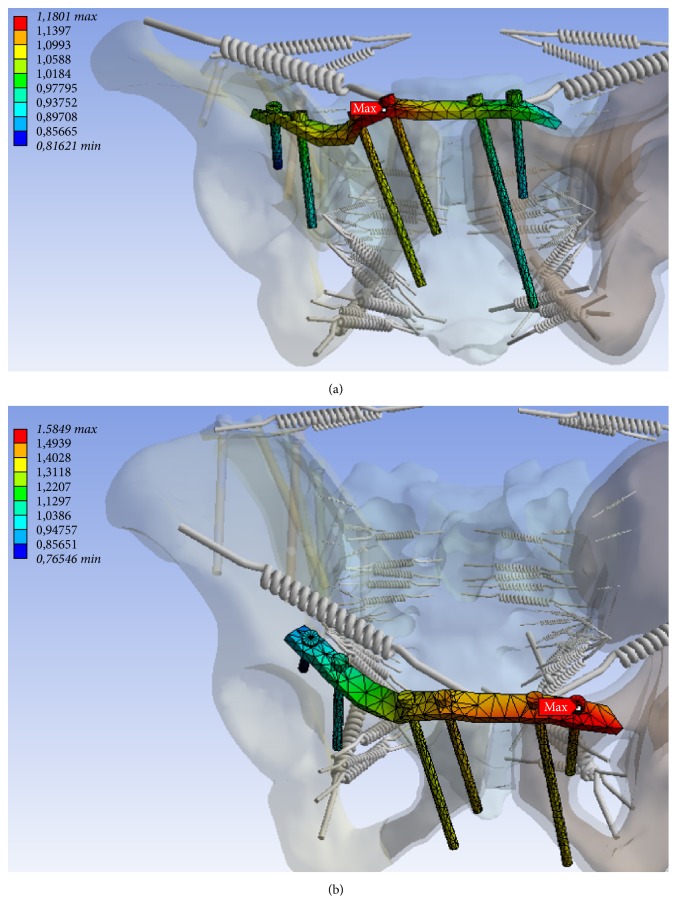
Introduction. The main purpose of this study is to develop an efficient technique for generating FE models of pelvic ring fractures that is capable of predicting possible failure regions of osteosynthesis with acceptable accuracy. Methods. Patient-specific FE models of two patients with osteoporotic pelvic fractures were generated. A validated FE model of an uninjured pelvis from our previous study was used as a master model. Then, fracture morphologies and implant positions defined by a trauma surgeon in the preoperative CT were manually introduced as 3D splines to the master model. Four loading cases were used as boundary conditions. Regions of high stresses in the models were compared with actual locations of implant breakages and loosening identified from follow-up X-rays. Results. Model predictions and the actual clinical outcomes matched well. For Patient A, zones of increased tension and maximum stress coincided well with the actual locations of implant loosening. For Patient B, the model predicted accurately the loosening of the implant in the anterior region. Conclusion. Since a significant reduction in time and labour was achieved in our mesh generation technique, it can be considered as a viable option to be implemented as a part of the clinical routine to aid presurgical planning and postsurgical management of pelvic ring fracture patients.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Williams R. P., Friis E. A., Cooke F. W., McQueen D. A., Toohey J. S. External fixation of unstable malgaigne fractures: the comparative mechanical performance of a new configuration. Orthopaedic Review. 1992;21(12):1423–1430. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
