

Adult infiltrating gliomas with WHO 2016 integrated diagnosis: additional prognostic roles of ATRX and TERT
- PMID: 28255664
- PMCID: PMC5432658
- DOI: 10.1007/s00401-017-1690-1
Adult infiltrating gliomas with WHO 2016 integrated diagnosis: additional prognostic roles of ATRX and TERT
Abstract
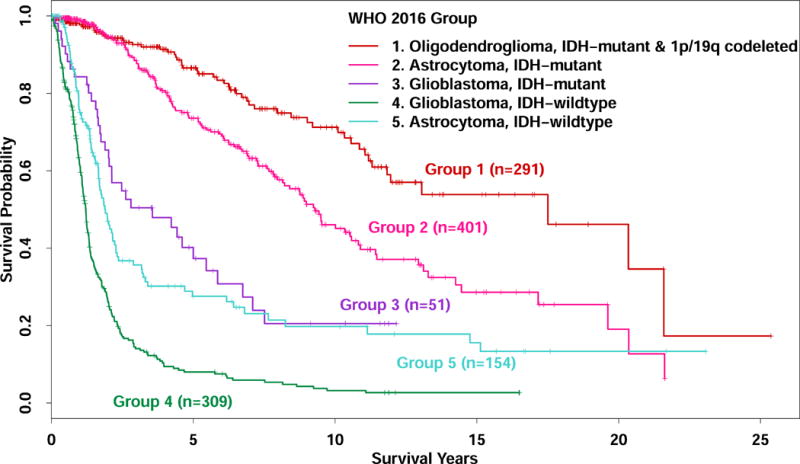
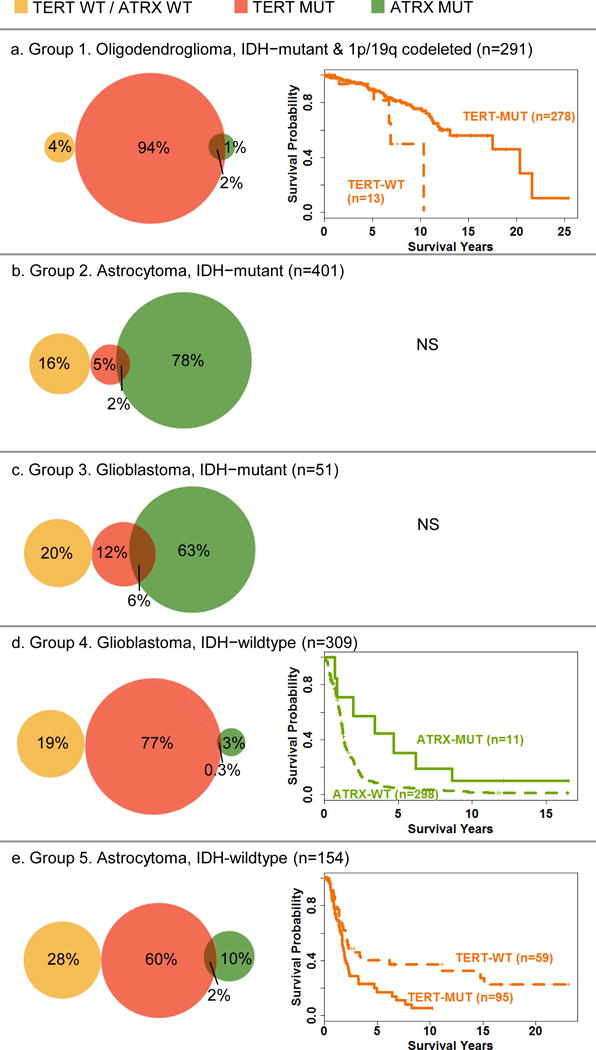
The "integrated diagnosis" for infiltrating gliomas in the 2016 revised World Health Organization (WHO) classification of tumors of the central nervous system requires assessment of the tumor for IDH mutations and 1p/19q codeletion. Since TERT promoter mutations and ATRX alterations have been shown to be associated with prognosis, we analyzed whether these tumor markers provide additional prognostic information within each of the five WHO 2016 categories. We used data for 1206 patients from the UCSF Adult Glioma Study, the Mayo Clinic and The Cancer Genome Atlas (TCGA) with infiltrative glioma, grades II-IV for whom tumor status for IDH, 1p/19q codeletion, ATRX, and TERT had been determined. All cases were assigned to one of 5 groups following the WHO 2016 diagnostic criteria based on their morphologic features, and IDH and 1p/19q codeletion status. These groups are: (1) Oligodendroglioma, IDH-mutant and 1p/19q-codeleted; (2) Astrocytoma, IDH-mutant; (3) Glioblastoma, IDH-mutant; (4) Glioblastoma, IDH-wildtype; and (5) Astrocytoma, IDH-wildtype. Within each group, we used univariate and multivariate Cox proportional hazards models to assess associations of overall survival with patient age at diagnosis, grade, and ATRX alteration status and/or TERT promoter mutation status. Among Group 1 IDH-mutant 1p/19q-codeleted oligodendrogliomas, the TERT-WT group had significantly worse overall survival than the TERT-MUT group (HR: 2.72, 95% CI 1.05-7.04, p = 0.04). In both Group 2, IDH-mutant astrocytomas and Group 3, IDH-mutant glioblastomas, neither TERT mutations nor ATRX alterations were significantly associated with survival. Among Group 4, IDH-wildtype glioblastomas, ATRX alterations were associated with favorable outcomes (HR: 0.36, 95% CI 0.17-0.81, p = 0.01). Among Group 5, IDH-wildtype astrocytomas, the TERT-WT group had significantly better overall survival than the TERT-MUT group (HR: 0.48, 95% CI 0.27-0.87), p = 0.02). Thus, we present evidence that in certain WHO 2016 diagnostic groups, testing for TERT promoter mutations or ATRX alterations may provide additional useful prognostic information.
Keywords: ATRX alteration; Brain tumor prognosis; Glioma classification; TERT promoter mutation; Telomere maintenance.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, Ohno M, Collins VP, Kawahara N, et al. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013;126:267–276. doi: 10.1007/s00401-013-1141-6. - DOI - PubMed
-
- Arita H, Yamasaki K, Matsushita Y, Nakamura T, Shimokawa A, Takami H, Tanaka S, Mukasa A, Shirahata M, Shimizu S, et al. A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas. Acta Neuropathol Commun. 2016;4:79. doi: 10.1186/s40478-016-0351-2. - DOI - PMC - PubMed
-
- Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA, Morozova O, Newton Y, Radenbaugh A, Pagnotta SM, et al. Molecular Profiling Reveals Biologically Discrete Subsets and Pathways of Progression in Diffuse Glioma. Cell. 2016;164:550–563. doi: 10.1016/j.cell.2015.12.028. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA139020/CA/NCI NIH HHS/United States
- HHSN261201000140C/CA/NCI NIH HHS/United States
- P50 CA108961/CA/NCI NIH HHS/United States
- RC1 NS068222/NS/NINDS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R25 CA112355/CA/NCI NIH HHS/United States
- R01 CA126831/CA/NCI NIH HHS/United States
- P50 CA097257/CA/NCI NIH HHS/United States
- U58 DP003862/DP/NCCDPHP CDC HHS/United States
- KL2 TR001862/TR/NCATS NIH HHS/United States
- R01 CA052689/CA/NCI NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- P30 CA082103/CA/NCI NIH HHS/United States
- P30 CA015083/CA/NCI NIH HHS/United States
- HHSN261201000035I/CA/NCI NIH HHS/United States
- HHSN261201000035C/PC/NCI NIH HHS/United States
- HHSN261201000034C/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
