

Clinical and pathological evolution of giant cell arteritis: a prospective study of follow-up temporal artery biopsies in 40 treated patients
- PMID: 28256573
- PMCID: PMC5650068
- DOI: 10.1038/modpathol.2017.10
Clinical and pathological evolution of giant cell arteritis: a prospective study of follow-up temporal artery biopsies in 40 treated patients
Abstract
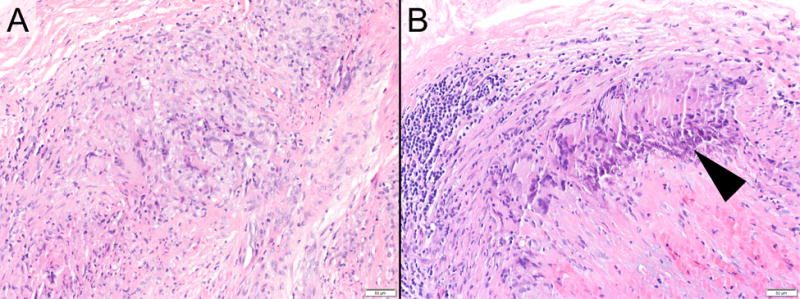
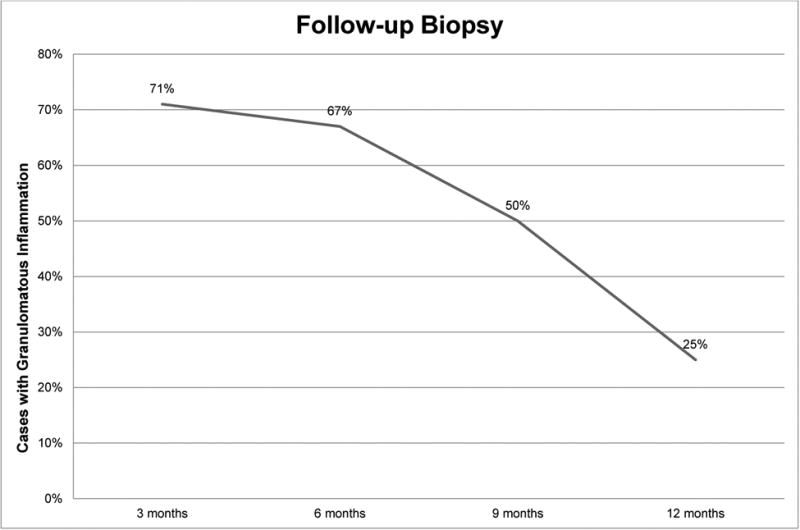
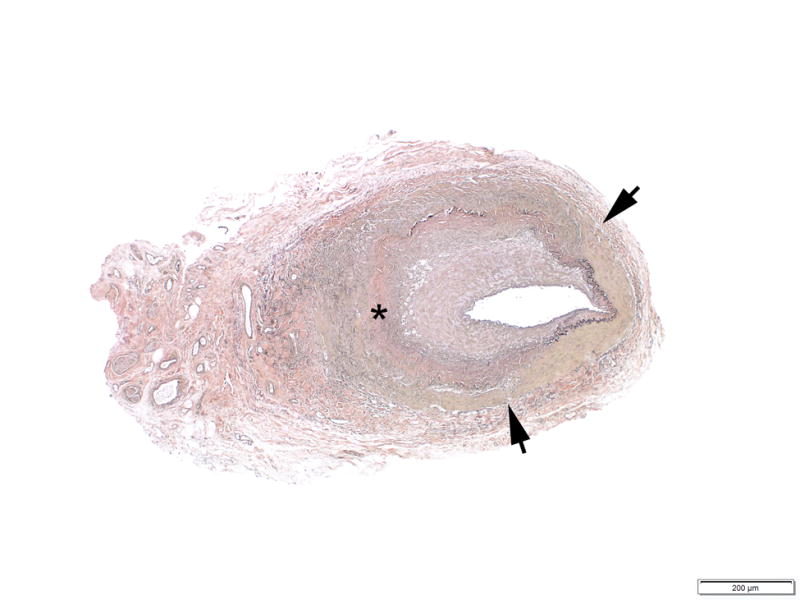
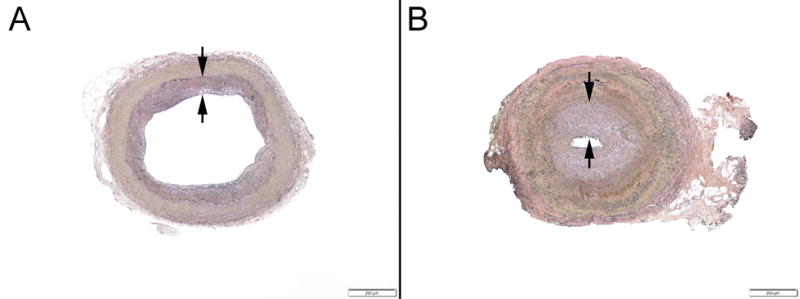
Although clinical signs and symptoms of giant cell arteritis improve promptly after starting glucocorticoid therapy, reports have suggested that the vascular inflammation may persist. To assess the duration and quality of histopathologic changes in treated patients, we prospectively obtained second temporal artery biopsies in patients treated for 3 to 12 months after their first diagnostic biopsy. Forty patients (28 women, 12 men, median age 77 years) agreed to have a second temporal artery biopsy randomly assigned to 3, 6, 9, or 12 months subsequent to the first. Clinical and laboratory evaluation of the patient cohort revealed a typical rapid response and continued suppression of clinical manifestations as a result of glucocorticoid treatment. Histopathologic findings, evaluated in a blinded manner by a cardiovascular pathologist, showed unequivocal findings of vasculitis in 7/10 patients with second temporal artery biopsy at 3 months, 9/12 at 6 months, 4/9 at 9 months, and 4/9 at 12 months. Lymphocytes were present in all positive initial biopsies and remained the dominant cell population in chronically treated patients. Granulomatous inflammation decreased in a time-dependent manner from 78 to 100% at initial biopsy to 50% at 9 months and 25% at 12 months. The increased medial fibrosis noted in the second biopsies (60 vs 33% in primary temporal artery biopsies) suggested that the finding may represent a chronic finding in arteritis. In summary, the response to glucocorticoids in giant cell arteritis was frequently discordant. Clinical manifestations were readily suppressed, but vascular changes were gradual and often incomplete.
Conflict of interest statement
Figures
References
-
- Aiello PD, Trautmann JC, McPhee TJ, Kunselman AR, Hunder GG. Visual prognosis in giant cell arteritis. Ophthalmology. 1993;100(4):550–555. - PubMed
-
- Evans JM, Batts KP, Hunder GG. Persistent giant cell arteritis despite corticosteroid treatment. Mayo Clin Proc. 1994;69:1060–1061. - PubMed
-
- Weyand CM, Goronzy JJ. Giant cell arteritis as an antigen-driven disease. Rheum Dis Clin North Am. 1995;21:1027–1039. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
