

MR imaging in patients with male-to-female sex reassignment surgery: postoperative anatomy and complications
- PMID: 28256903
- PMCID: PMC5605084
- DOI: 10.1259/bjr.20170062
MR imaging in patients with male-to-female sex reassignment surgery: postoperative anatomy and complications
Abstract
Objective: To investigate the role of MRI in the evaluation of both the new female anatomy and complications in male-to-female sex reassignment surgery (MtF-SRS).
Methods: 71 consecutive patients with MtF-SRS had 74 MRI [age range, 21-63 years; mean (±standard deviation) age, 36 ± 10 years; median age, 37 years]. In 47 patients, MRI was performed to rule out early post-operative complications after gender conversion (n = 40), vaginoplasty (n = 6) or remodelling of the labia majora (n = 1). In 27 patients, MRI was performed 1-20 years after MtF-SRS for late post-operative complications, pain or dysuria, inflammatory changes or poor cosmetic outcome. Three patients had MRI both before and after the operation.
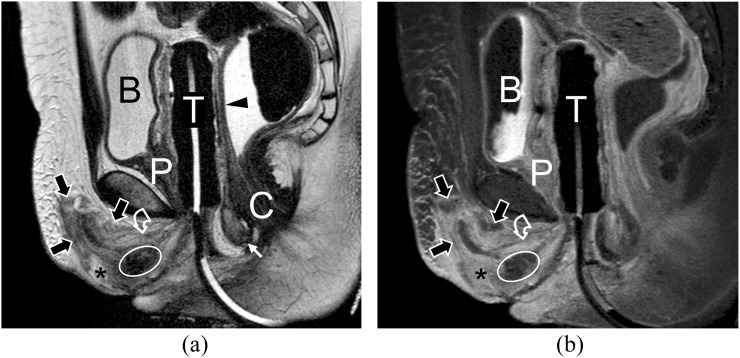
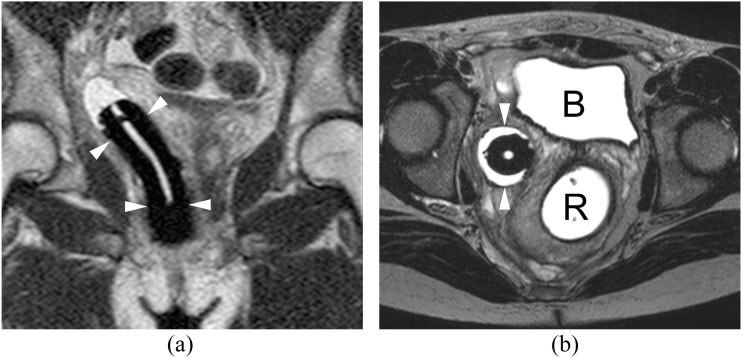
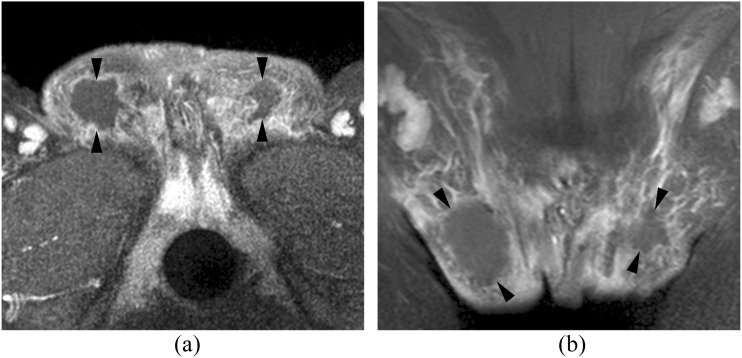
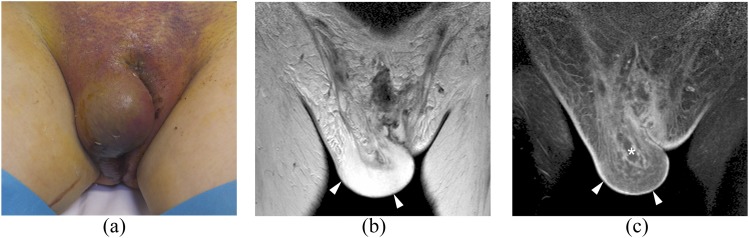
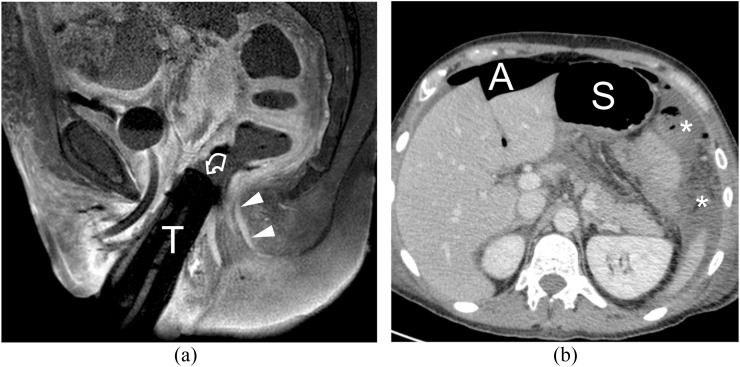
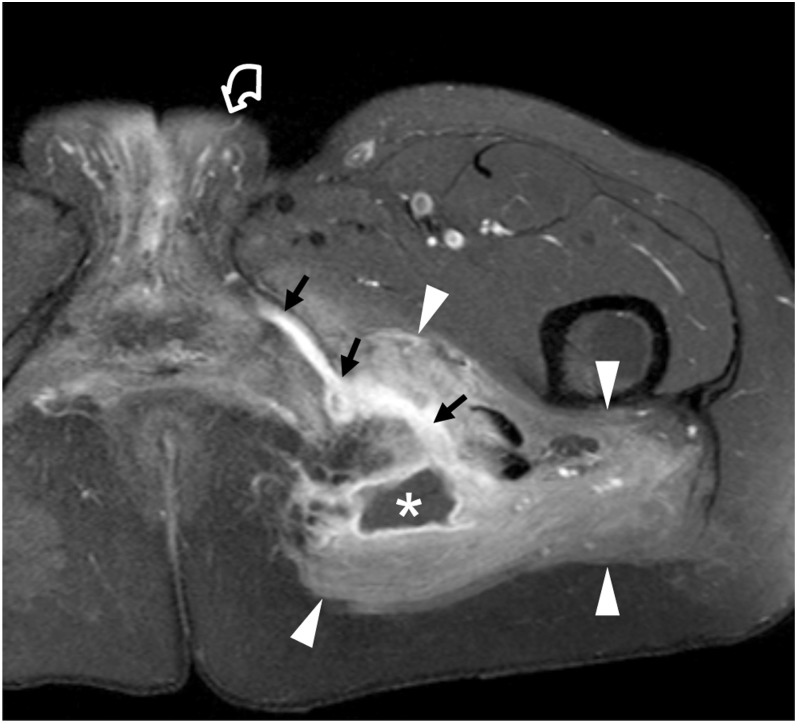
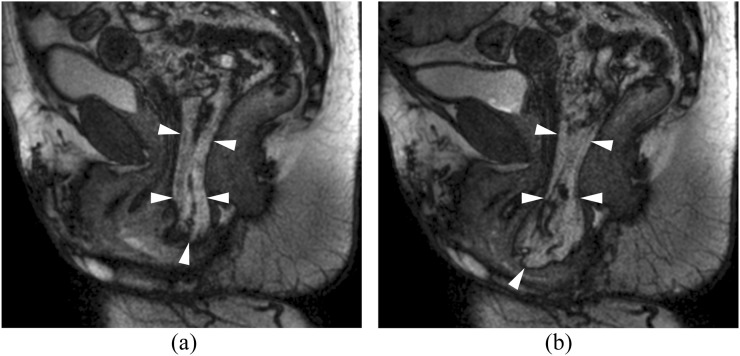
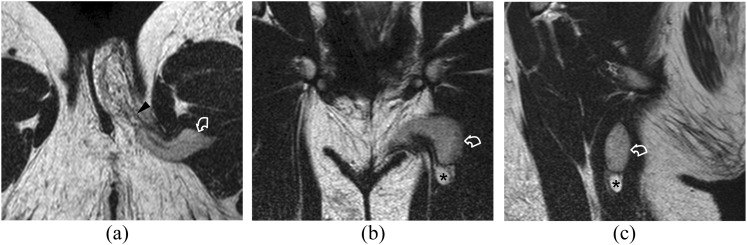
Results: MRI allowed investigation of the new female anatomy in all cases. Soon after MtF-SRS, a small amount of blood was identified in all patients around the neoclitoris, urethral plaque and labia. Post-operative complications were clinically significant fluid collections (n = 5), labial abscesses (n = 2), severe cellulitis (n = 3), partial neovaginal prolapse (n = 3), focal necrosis and dehiscence of the vaginal wall (n = 2) and hypovascularization of the neoclitoris (n = 1). After ileal vaginoplasty, three patients developed clinically insignificant haematomas, one a large rectovaginal fistula with dehiscence of the intestinal anastomosis and bowel perforation (n = 1). In the 27 patients investigated 1-20 years after MfF-SRS, MRI demonstrated cavernosal remnants (n = 10), spared testis (n = 1) neovaginal strictures (n = 8), fistulas and abscesses (n = 3) and prolapse (n = 2). Three of these patients also had fibrotic changes. In the remaining three patients, no pathological features were identified.
Conclusion: After genital reconfiguration, MRI allows assessment of the post-operative anatomy and of post-operative complications. Advances in knowledge: Imaging features of the new anatomy and of surgical complications after SRS are discussed and illustrated.
Figures




References
-
- Krege S, Bex A, Lümmen G, Rübben H. Male-to-female transsexualism: a technique, results and long-term follow-up in 66 patients. BJU Int 2001; 88: 396–402. - PubMed
-
- Rossi Neto R, Hintz F, Krege S, Rübben H, Vom Dorp F. Gender reassignment surgery—a 13 year review of surgical outcomes. Int Braz J Urol 2012; 38: 97–107. doi: https://doi.org/10.1590/s1677-55382012000100014 - DOI - PubMed
-
- Cova M, Mosconi E, Liguori G, Bucci S, Trombetta C, Belgrano E, et al. . Value of magnetic resonance imaging in the evaluation of sex-reassignment surgery in male-to-female transsexuals. Abdom Imaging 2003; 28: 728–32. doi: https://doi.org/10.1007/s00261-002-0100-9 - DOI - PubMed
-
- Trombetta C, Liguori G, Bucci S. Radiological evaluation of vaginal width and depth in male-to-female transsexuals by the use of magnetic resonance imaging. World J Urol 2004; 22: 405–8. doi: https://doi.org/10.1007/s00345-004-0422-z - DOI - PubMed
-
- Brunocilla E, Soli M, Franceschelli A, Schiavina R, Borghesi M, Gentile G, et al. . Radiological evaluation by magnetic resonance of the “new anatomy” of transsexual patients undergoing male to female sex reassignment surgery. Int J Impot Res 2012; 24: 206–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
