

Serial Procalcitonin Predicts Mortality in Severe Sepsis Patients: Results From the Multicenter Procalcitonin MOnitoring SEpsis (MOSES) Study
- PMID: 28257335
- PMCID: PMC5389588
- DOI: 10.1097/CCM.0000000000002321
Serial Procalcitonin Predicts Mortality in Severe Sepsis Patients: Results From the Multicenter Procalcitonin MOnitoring SEpsis (MOSES) Study
Abstract
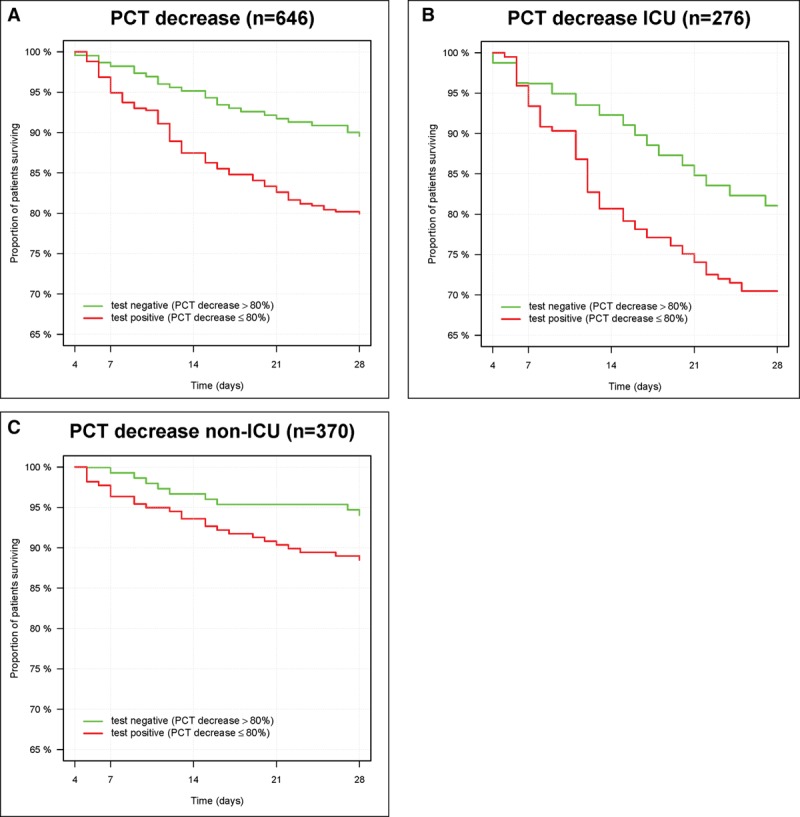
Objectives: To prospectively validate that the inability to decrease procalcitonin levels by more than 80% between baseline and day 4 is associated with increased 28-day all-cause mortality in a large sepsis patient population recruited across the United States.
Design: Blinded, prospective multicenter observational clinical trial following an Food and Drug Administration-approved protocol.
Setting: Thirteen U.S.-based emergency departments and ICUs.
Patients: Consecutive patients meeting criteria for severe sepsis or septic shock who were admitted to the ICU from the emergency department, other wards, or directly from out of hospital were included.
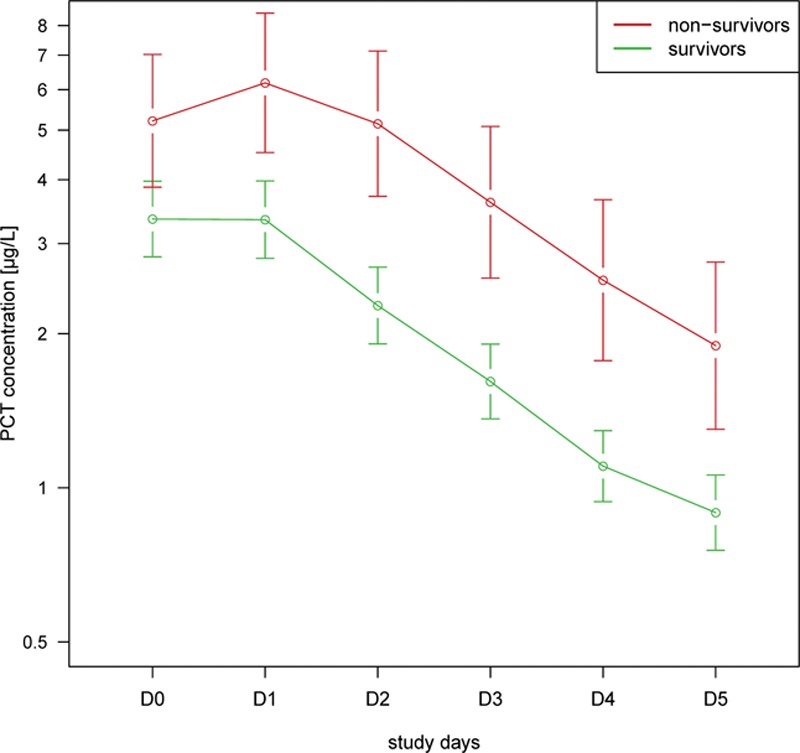
Interventions: Procalcitonin was measured daily over the first 5 days.
Measurements and main results: The primary analysis of interest was the relationship between a procalcitonin decrease of more than 80% from baseline to day 4 and 28-day mortality using Cox proportional hazards regression. Among 858 enrolled patients, 646 patients were alive and in the hospital on day 4 and included in the main intention-to-diagnose analysis. The 28-day all-cause mortality was two-fold higher when procalcitonin did not show a decrease of more than 80% from baseline to day 4 (20% vs 10%; p = 0.001). This was confirmed as an independent predictor in Cox regression analysis (hazard ratio, 1.97 [95% CI, 1.18-3.30; p < 0.009]) after adjusting for demographics, Acute Physiology and Chronic Health Evaluation II, ICU residence on day 4, sepsis syndrome severity, antibiotic administration time, and other relevant confounders.
Conclusions: Results of this large, prospective multicenter U.S. study indicate that inability to decrease procalcitonin by more than 80% is a significant independent predictor of mortality and may aid in sepsis care.
Conflict of interest statement
Dr. Schuetz received support from B·R·A·H·M·S GmbH and bioMérieux to attend meetings and fulfill speaking engagements and received research grants from these two firms. Dr. Birkhahn’s institution received funding from Alere. Dr. Singer received support for article research from Thermo Fisher Scientific. Dr. Runyon’s institution received funding from National Institute of General Medical Sciences of the National Institutes of Health (NIH), Center for Disease Control and Prevention, and National Highway Traffic Safety Administration. He disclosed other support from MedEvac Foundation, Carolinas Trauma Network Research Center of Excellence, Janssen Pharmaceutical Companies, Emergency MCG USA, Siemens Healthcare Diagnostics, Boehringer Ingelheim Pharmaceuticals, Trinity Biotech, Durata Therapeutics International, Abbott Fund, and Bristol- Myers Squibb. Dr. Self received funding from B·R·A·H·M·S/ThermoFisher (funding to conduct the study reported in this article). He received funding from Bio-Fire (consultant fees), Abbott POC (consultant fee), and Venaxis (consultant fees). He disclosed other support from Pfizer (funding for clinical research), Venaxis (funding for clinical research), RPS (funding for clinical research), Kypha (funding for clinical research), and BioAegis (funding for clinical research). He received support for article research from the NIH. Drs. Ebmeyer, Johannes, Wiemer, and Schwabe are employees of B·R·A·H·M·S GmbH, which is the company that sponsored the trial reported in this article and manufacturer of B·R·A·H·M·S PCT sensitive Kryptor. Dr. Shapiro has received consulting and speaking fees from B·R·A·H·M·S GmbH and Siemens Medical. He received funding from Cheetah Medical and Cumberland Pharma. He disclosed other support from rapid pathogen screening and nanomix. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Procalcitonin Clearance and Prognosis in Sepsis: Are There Really an Optimal Cutoff and Time Interval?Crit Care Med. 2017 Oct;45(10):e1097-e1098. doi: 10.1097/CCM.0000000000002552. Crit Care Med. 2017. PMID: 28915193 No abstract available.
-
The authors reply.Crit Care Med. 2017 Oct;45(10):e1098-e1099. doi: 10.1097/CCM.0000000000002608. Crit Care Med. 2017. PMID: 28915194 No abstract available.
-
Potential Confounders of Procalcitonin-Guided Antibiotic Therapy for Sepsis.Crit Care Med. 2017 Dec;45(12):e1310-e1311. doi: 10.1097/CCM.0000000000002713. Crit Care Med. 2017. PMID: 29149015 No abstract available.
-
Implications of Procalcitonin Testing in Critically Ill Patients with Sepsis.Am J Respir Crit Care Med. 2019 Jan 15;199(2):232-234. doi: 10.1164/rccm.201712-2544RR. Am J Respir Crit Care Med. 2019. PMID: 30423258 No abstract available.
References
-
- Ouanes I, Schwebel C, Français A, et al. Outcomerea Study Group: A model to predict short-term death or readmission after intensive care unit discharge. J Crit Care 2012; 27:422.e1–422.e9 - PubMed
-
- Jun KR, Lee JN, Song SA, et al. Serial changes in serum procalcitonin, interleukin 6, and C-reactive protein levels according to non-specific surgical stimulation. Clin Chem Lab Med 2015; 53:549–558 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
