

Uncovering precision phenotype-biomarker associations in traumatic brain injury using topological data analysis
- PMID: 28257413
- PMCID: PMC5336356
- DOI: 10.1371/journal.pone.0169490
Uncovering precision phenotype-biomarker associations in traumatic brain injury using topological data analysis
Abstract
Background: Traumatic brain injury (TBI) is a complex disorder that is traditionally stratified based on clinical signs and symptoms. Recent imaging and molecular biomarker innovations provide unprecedented opportunities for improved TBI precision medicine, incorporating patho-anatomical and molecular mechanisms. Complete integration of these diverse data for TBI diagnosis and patient stratification remains an unmet challenge.
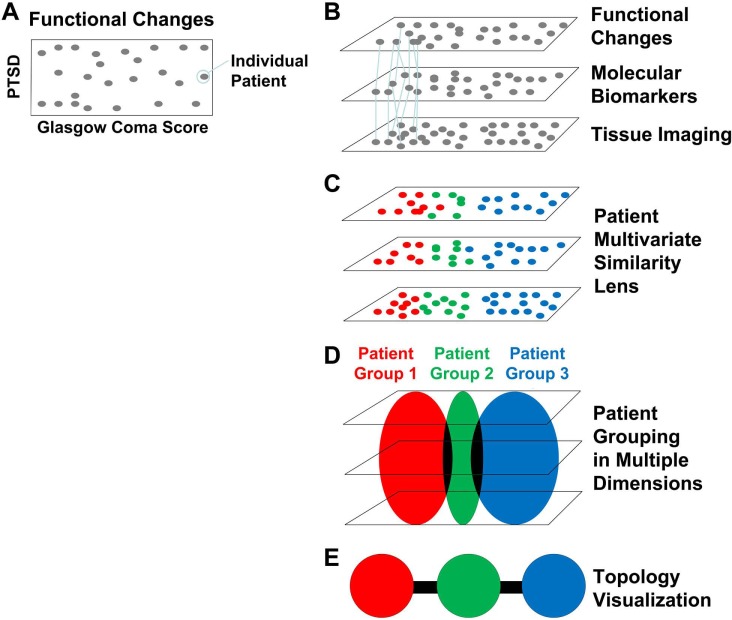
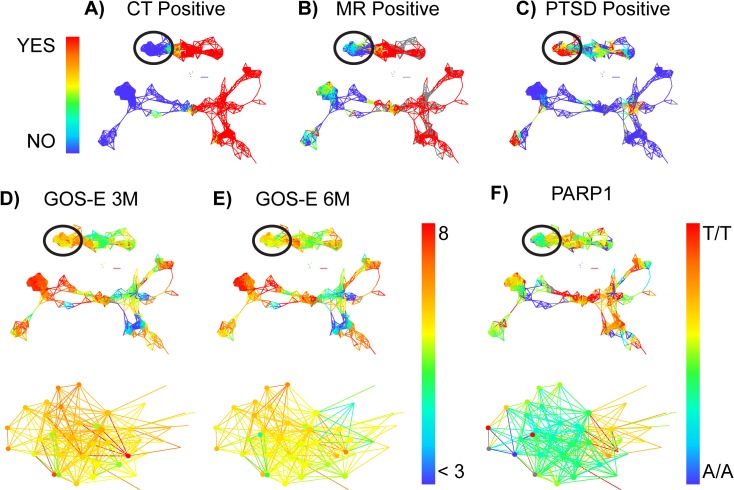
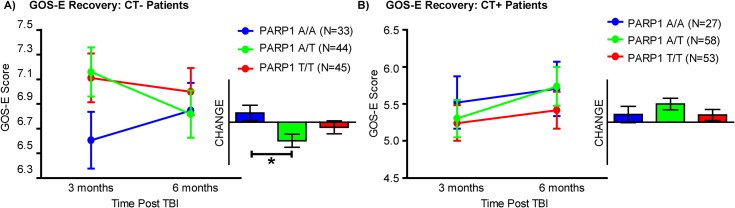
Methods and findings: The Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Pilot multicenter study enrolled 586 acute TBI patients and collected diverse common data elements (TBI-CDEs) across the study population, including imaging, genetics, and clinical outcomes. We then applied topology-based data-driven discovery to identify natural subgroups of patients, based on the TBI-CDEs collected. Our hypothesis was two-fold: 1) A machine learning tool known as topological data analysis (TDA) would reveal data-driven patterns in patient outcomes to identify candidate biomarkers of recovery, and 2) TDA-identified biomarkers would significantly predict patient outcome recovery after TBI using more traditional methods of univariate statistical tests. TDA algorithms organized and mapped the data of TBI patients in multidimensional space, identifying a subset of mild TBI patients with a specific multivariate phenotype associated with unfavorable outcome at 3 and 6 months after injury. Further analyses revealed that this patient subset had high rates of post-traumatic stress disorder (PTSD), and enrichment in several distinct genetic polymorphisms associated with cellular responses to stress and DNA damage (PARP1), and in striatal dopamine processing (ANKK1, COMT, DRD2).
Conclusions: TDA identified a unique diagnostic subgroup of patients with unfavorable outcome after mild TBI that were significantly predicted by the presence of specific genetic polymorphisms. Machine learning methods such as TDA may provide a robust method for patient stratification and treatment planning targeting identified biomarkers in future clinical trials in TBI patients.
Trial registration: ClinicalTrials.gov Identifier NCT01565551.
Conflict of interest statement
Figures
References
-
- CDC. TBI: Get the Facts | Concussion | Traumatic Brain Injury | CDC Injury Center [Internet]. Available: http://www.cdc.gov/TraumaticBrainInjury/get_the_facts.html
-
- Viano DC, Casson IR, Pellman EJ, Zhang L, King AI, Yang KH. Concussion in professional football: brain responses by finite element analysis: part 9. Neurosurgery. 2005;57: 891-916-916. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
