

Non-contraceptive oestrogen-containing preparations for controlling symptoms of premenstrual syndrome
- PMID: 28257559
- PMCID: PMC6464572
- DOI: 10.1002/14651858.CD010503.pub2
Non-contraceptive oestrogen-containing preparations for controlling symptoms of premenstrual syndrome
Abstract
Background: Premenstrual syndrome (PMS) is a psychological and somatic disorder of unknown aetiology, with symptoms typically including irritability, depression, mood swings, bloating, breast tenderness and sleep disturbances. About 3% to 10% of women who experience these symptoms may also meet criteria for premenstrual dysphoric disorder (PMDD). PMS symptoms recur during the luteal phase of the menstrual cycle and reduce by the end of menstruation. PMS results from ovulation and may be due to ovarian steroid interactions relating to neurotransmitter dysfunction. Premenstrual disorders have a devastating effect on women, their families and their work.Several treatment options have been suggested for PMS, including pharmacological and surgical interventions. The treatments thought to be most effective tend to fall into one of two categories: suppressing ovulation or correcting a speculated neuroendocrine anomaly.Transdermal oestradiol by patch, gel or implant effectively stops ovulation and the cyclical hormonal changes which produce the cyclical symptoms. These preparations are normally used for hormone therapy and contain lower doses of oestrogen than found in oral contraceptive pills. A shortened seven-day course of a progestogen is required each month for endometrial protection but can reproduce premenstrual syndrome-type symptoms in these women.
Objectives: To determine the effectiveness and safety of non-contraceptive oestrogen-containing preparations in the management of PMS.
Search methods: On 14 March 2016, we searched the following databases: the Cochrane Gynaecology and Fertility Group (CGF) Specialised Register; Cochrane Central Register of Studies (CRSO); MEDLINE; Embase; PsycINFO; CINAHL; ClinicalTrials.gov; metaRegister of Controlled trials (mRCT); and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) Search Portal. In addition, we checked the reference lists of articles retrieved.
Selection criteria: We included published and unpublished randomized placebo or active controlled trials on the efficacy of the use of non-contraceptive oestrogen-containing preparations in the management of premenstrual syndrome in women of reproductive age with PMS diagnosed by at least two prospective cycles without current psychiatric disorder.
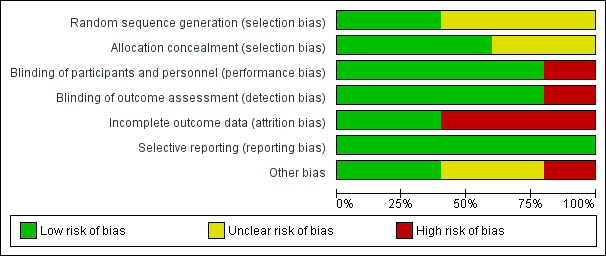
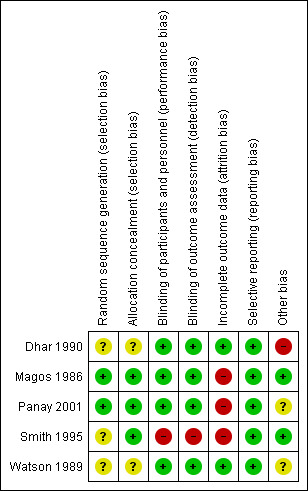
Data collection and analysis: Two review authors independently selected studies, assessed risk of bias, extracted data on premenstrual symptoms and adverse effects and entered data into Review Manager 5 software. Where possible, intention-to-treat or modified intention-to-treat analysis was used. Studies were pooled using a fixed-effect model, analysing cross-over trials as parallel trials. Standardised mean differences (SMDs) with 95% confidence intervals (CIs) were calculated for premenstrual symptom scores. Risk ratios (RRs) with 95% confidence intervals (CIs) were calculated for dichotomous outcomes. The overall quality of the evidence was assessed using the GRADE working group methods.
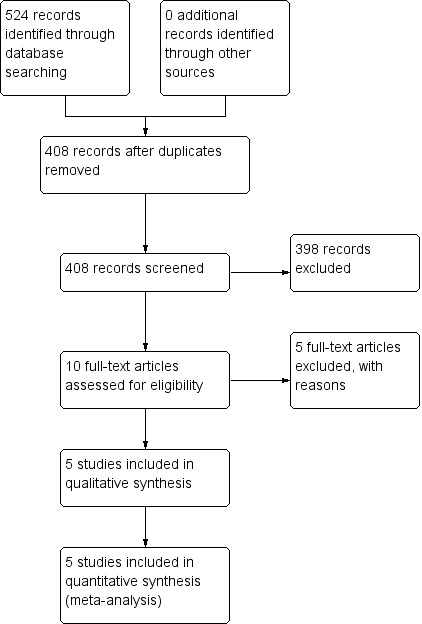
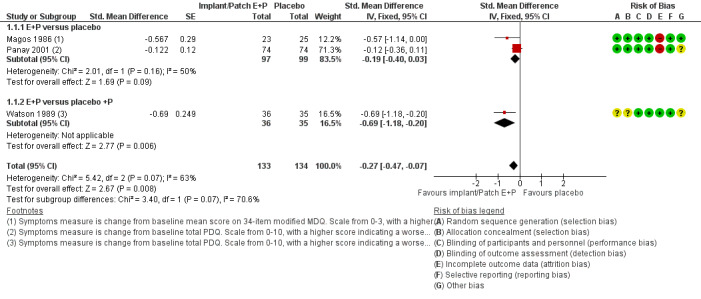
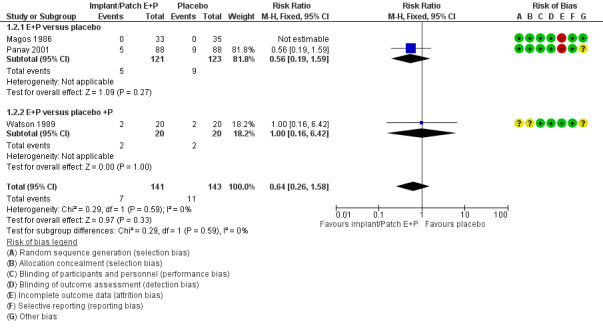
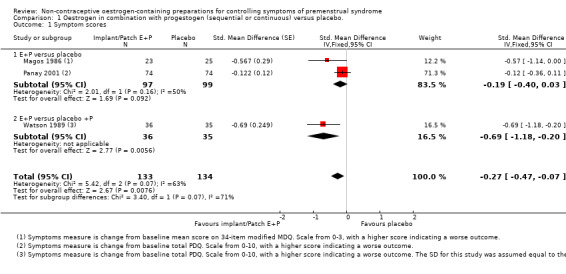
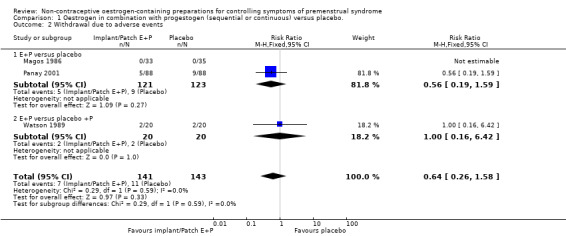
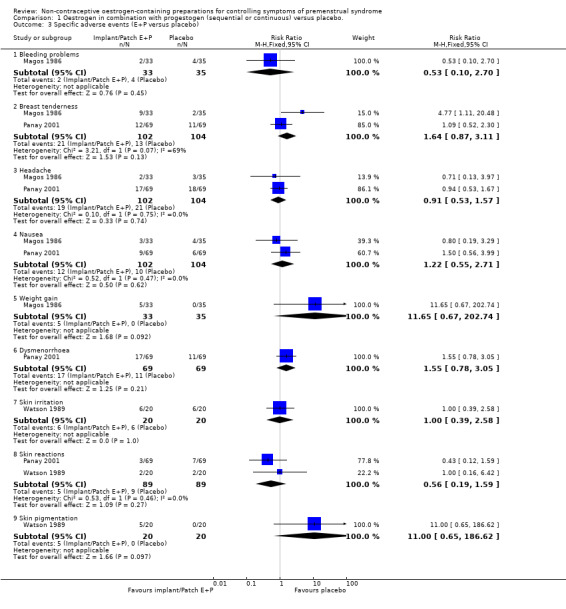
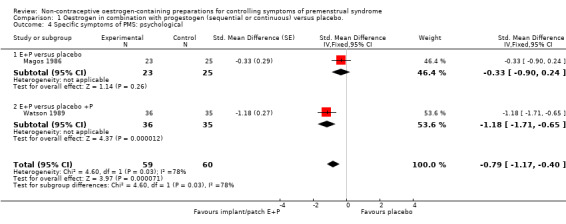
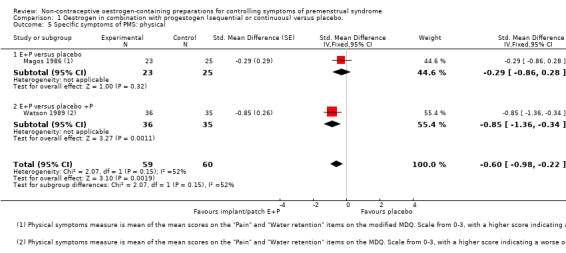
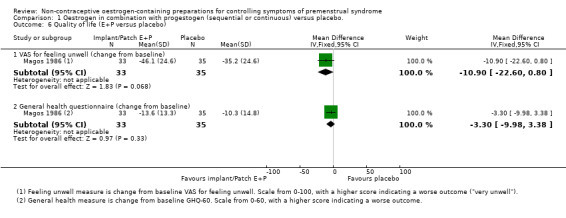
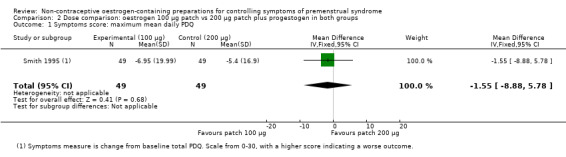
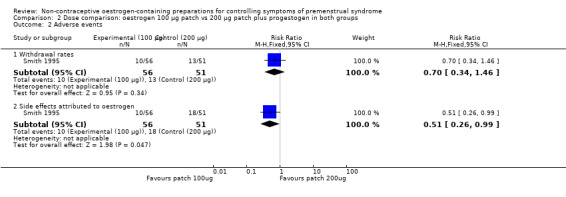
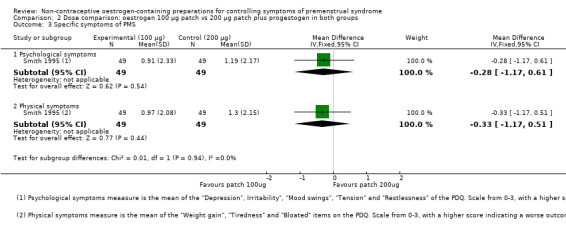
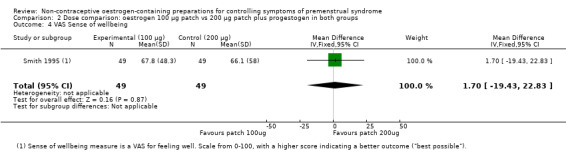
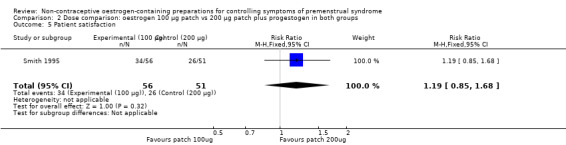
Main results: The search resulted in 524 potentially relevant articles. Five eligible randomized controlled trials (RCTs) were identified (305 women). Trials using oral tablets, transdermal patches and implants were identified. No trial used gels.One small cross-over trial (11 women, effective sample size 22 women considering cross-over trials) compared oral luteal-phase oestrogen versus placebo. Data were very low quality and unsuitable for analysis, but study authors reported that the intervention was ineffective and might aggravate the symptoms of PMS. They also reported that there were no adverse events.Three studies compared continuous oestrogen with progestogen versus placebo (with or without progestogen). These trials were of reasonable quality, although with a high risk of attrition bias and an unclear risk of bias due to potential carry-over effects in two cross-over trials. Continuous oestrogen had a small to moderate positive effect on global symptom scores (SMD -0.34, 95% CI -0.59 to -0.10, P = 0.005, 3 RCTs, 158 women, effective sample size 267 women, I² = 63%, very low quality evidence). The evidence was too imprecise to determine if the groups differed in withdrawal rates due to adverse effects (RR 0.64, 95% CI 0.26 to 1.58, P = 0.33, 3 RCTs, 196 women, effective sample size 284 women, I² = 0%, very low quality evidence). Similarly, the evidence was very imprecise in measures of specific adverse events, with large uncertainties around the true value of the relative risk. None of the studies reported on long-term risks such as endometrial cancer or breast cancer.One study compared patch dosage (100 vs 200 µg oestrogen, with progestogen in both arms) and had a high risk of performance bias, detection bias and attrition bias. The study did not find evidence that dosage affects global symptoms but there was much uncertainty around the effect estimate (SMD -1.55, 95% CI -8.88 to 5.78, P = 0.68, 1 RCT, 98 women, very low quality evidence). The evidence on rates of withdrawal for adverse events was too imprecise to draw any conclusions (RR 0.70, 95% CI 0.34 to 1.46, P = 0.34, 1 RCT, 107 women, low-quality evidence). However, it appeared that the 100 µg dose might be associated with a lower overall risk of adverse events attributed to oestrogen (RR 0.51, 95% Cl 0.26 to 0.99, P = 0.05, 1 RCT, 107 women, very low quality evidence) with a large uncertainty around the effect estimate.The overall quality of the evidence for all comparisons was very low, mainly due to risk of bias (specifically attrition), imprecision, and statistical and clinical heterogeneity.
Authors' conclusions: We found very low quality evidence to support the effectiveness of continuous oestrogen (transdermal patches or subcutaneous implants) plus progestogen, with a small to moderate effect size. We found very low quality evidence from a study based on 11 women to suggest that luteal-phase oral unopposed oestrogen is probably ineffective and possibly detrimental for controlling the symptoms of PMS. A comparison between 200 µg and 100 µg doses of continuous oestrogen was inconclusive with regard to effectiveness, but suggested that the lower dose was less likely to cause side effects. Uncertainty remains regarding safety, as the identified studies were too small to provide definite answers. Moreover, no included trial addressed adverse effects that might occur beyond the typical trial duration of 2-8 months. This suggests the choice of oestrogen dose and mode of administration could be based on an individual woman's preference and modified according to the effectiveness and tolerability of the chosen regimen.
Conflict of interest statement
BN, JHK, OAU and FO have no interests to declare. PMSO has received some travel expenses, lecture fees and consultancy fees from Bayer Women’s Health, Abbvie Pharma, Umecrine Mood and Asarina Pharma for his work related to premenstrual disorders but on topics unrelated to the use of non‐contraceptive oestrogens in PMS.
Figures
Update of
References
References to studies included in this review
Dhar 1990 {published data only}
-
- Dhar V, Murphy BE. Double‐blind randomized crossover trial of luteal phase estrogens (Premarin) in the premenstrual syndrome (PMS). Psychoneuroendocrinology 1990;15(5‐6):489‐93. - PubMed
Magos 1986 {published data only}
Panay 2001 {unpublished data only}
-
- Panay N, Rees M, Domoney C, Zakaria F, Guilford S, Studd JW. A multicentre double‐blind crossover study comparing 100μg transdermal oestradiol with placebo in the treatment of severe premenstrual syndrome. British Menopause Society Journal 2001;7(Suppl 3):19‐20.
Smith 1995 {published data only}
-
- Smith RN, Studd JW, Zamblera D, Holland EF. A randomised comparison over 8 months of 100 micrograms and 200 micrograms twice weekly doses of transdermal oestradiol in the treatment of severe premenstrual syndrome. British Journal of Obstetrics and Gynaecology 1995;102(6):475‐84. [PUBMED: 7632640] - PubMed
Watson 1989 {published data only}
-
- Watson NR, Studd JWW. Treatment of severe premenstrual syndrome with oestradiol patches and cyclical oral norethisterone. Lancet 1989;334(8665):730‐2. - PubMed
References to studies excluded from this review
de Lignières 1986 {published data only}
Dennerstein 1988 {published data only}
-
- Dennerstein L, Morse C, Burrows G, Oats J, Brown J, Smith M. Menstrual migraine: a double‐blind trial of percutaneous estradiol. Gynecological Endocrinology 1988;2(2):113‐20. - PubMed
Domoney 2003 {published data only}
-
- Domoney C, Panay N, Hawkins A, Studd J. Treatment of premenstrual syndrome with transdermal oestrogen. International Journal of Gynaecology & Obstetrics 2003;83(suppl 3):37‐8.
Ensom 2003 {published data only}
-
- Ensom MH, Chong G, Zhou D, Beaudin B, Shalansky S, Bai TR. Estradiol in premenstrual asthma: a double‐blind, randomized, placebo‐controlled, crossover study. Pharmacotherapy 2003;23(5):561‐71. - PubMed
Halbreich 2012 {published data only}
-
- Halbreich U, Freeman EW, Rapkin AJ, Cohen LS, Grubb GS, Bergeron R, et al. Continuous oral levonorgestrel/ethinyl estradiol for treating premenstrual dysphoric disorder. Contraception 2012;85(1):19‐27. - PubMed
Additional references
Abraha 2010
ACOG 2001
-
- ACOG. ACOG practice bulletin: premenstrual syndrome. International Journal of Gynaecology and Obstetrics 2001;73:183‐91.
Atkins 2004
Deeks 2010
-
- Deeks JJ, Higgins JPT on behalf of the Statistical Methods Group of The Cochrane Collaboration. Statistical algorithms in Review Manager; August 2010. tech.cochrane.org/revman/documentation/statistical‐methods‐in‐revman‐5.pdf (accessed 11 January 2017).
DSM‐IV‐TR
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed.). 4th Edition. Arlington, VA: American Psychiatric Press, Inc., 2000.
Ford 2012
Gianetto‐Berruti 2002
-
- Gianetto‐Berruti A, Feyles V. Premenstrual syndrome. Minerva Ginecologica 2002;54(2):85‐95. - PubMed
GRADEpro GDT 2014 [Computer program]
-
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed prior to 4 November 2016. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Green 2017
-
- Green LJ, O’Brien PMS, Panay N, Craig M on behalf of the Royal College of Obstetricians and Gynaecologists. Management of premenstrual syndrome. Br J Obst Gynaecol 2017;124:e73‐e105.
Halbreich 2003
-
- Halbreich U, Borenstein J, Pearlstein T, Kahn LS. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD). Psychoneuroendocrinology 2003;28(Suppl 3):1‐23. - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
ISPMD 2011
Johnson 2004
-
- Johnson S. The epidemiology of premenstrual syndrome. Primary Psychiatry 2004;11(2):27‐32.
Kaur 2004
-
- Kaur G, Gonsalves L, Thacker HL. Premenstrual dysphoric disorder: a review for the treating practitioner. Cleveland Clinic Journal of Medicine 2004;71(4):303‐5, 312‐3, 317‐8 passim. - PubMed
Lopez 2012
Marjoribanks 2013
Moher 2009
Norman 2003
-
- Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health‐related quality of life: the remarkable universality of half a standard deviation. Medical Care 2003;41(3):582‐92. - PubMed
O'Brien 2003
-
- O'Brien P, Ismail K, Dimmock P. Premenstrual syndrome. In: Shaw R, Soutter W, Stanton S editor(s). Gynaecology. 3rd Edition. London: Churchill Livingston, 2003:401‐11.
O'Brien 2011
-
- O'Brien S, Rapkin A, Dennerstein L, Nevatte T. Diagnosis and Management of Premenstrual Syndrome. BMJ 2011;342:d2994. - PubMed
Panay 2005
-
- Panay N. Premenstrual syndrome: Making sense of the options. Pulse 2004;65(8):50‐4.
Rapkin 2007
-
- Rapkin AJ, Kuo J. The Premenstrual Syndromes. In: O’Brien PMS, Rapkin A, Schmidt P editor(s). PMS & PMDD. London: Informa Healthcare, 2007:69‐83.
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Roberts 2014
-
- Roberts HE, Hickey M, Lethaby A. Hormone therapy in postmenopausal women and risk of endometrial hyperplasia: A Cochrane review summary. Maturitas 2014;77(1):4‐6. [A Cochrane review summary. Maturitas,] - PubMed
Sackett 1996
-
- Sackett DL, Deeks JJ, Altman DG. Down with odds ratios!. Evidence Based Medicine 1996;1(6):164‐6.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical