

Biometry Characteristics in Adults and Children With Marfan Syndrome: From the Marfan Eye Consortium of Chicago
- PMID: 28257833
- PMCID: PMC5648325
- DOI: 10.1016/j.ajo.2017.02.022
Biometry Characteristics in Adults and Children With Marfan Syndrome: From the Marfan Eye Consortium of Chicago
Abstract
Purpose: To report on the biometric findings of adults and children with Marfan syndrome (MFS) recruited from 2 annual National Marfan Foundation conferences (2012 and 2015).
Design: Cross-sectional study.
Methods: Subjects diagnosed with MFS by Ghent 2 nosology were included for analysis. Subjects were divided into "adults" (≥16 years of age) and "children" (5-15 years of age). Biometric data included values for refractive error, axial length (AL), corneal curvature, anterior chamber depth, lens thickness, and central corneal thickness.
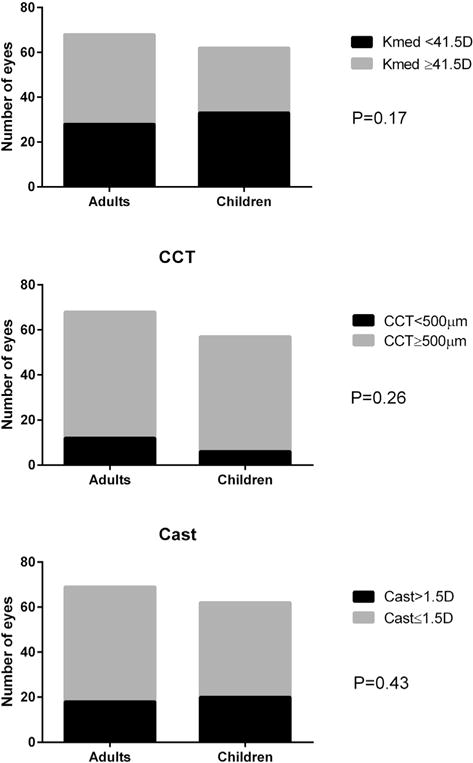
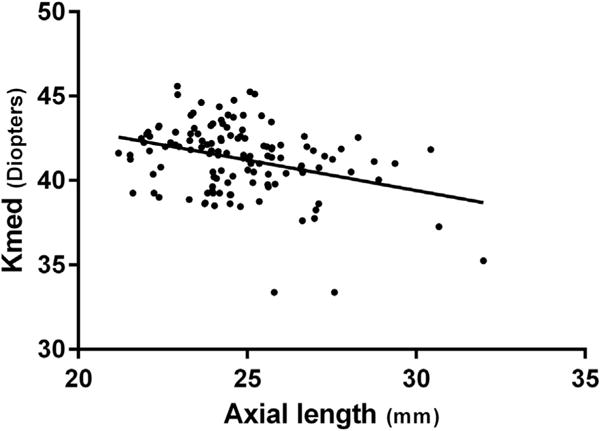
Results: Of the 117 subjects evaluated, 74 (35 adults, 32 children, and 7 children <5 years of age) had a definite diagnosis of MFS and were included in the study. The AL was longer (25.25 ± 0.32 mm vs 24.24 ± 0.33 mm, P = .03) and the lens was thicker (3.94 ± 0.09 mm vs 3.62 ± 0.10 mm, P = .03) in adults. Both groups had flat corneas (average keratometry [Kmed] of 41.59 ± 0.35 diopters [D] in adults vs 40.89 ± 0.36 D in children, P = .17). A negative correlation was found between AL and Kmed (-0.33, P < .001). The corneas of patients with MFS with ectopia lentis (EL) were significantly flatter and with higher degree of corneal astigmatism compared to patients without EL (Kmed of 40.68 ± 0.31 D vs 41.75 ± 0.28 D, P < .01 and corneal astigmatism of 1.68 ± 0.16 D vs 1.13 ± 0.14 D, P = .01).
Conclusions: Children with established MFS have flat corneas at least to the same degree as adults. Corneas of patients with MFS with EL are flatter and have a higher degree of corneal astigmatism. We strongly suggest that corneal parameters should be measured if MFS is suspected, especially in children that may not yet have developed EL.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE. Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet. 1996;62(4):417–426. - PubMed
-
- Loeys BL, Dietz HC, Braverman AC, et al. The revised Ghent nosology for the Marfan syndrome. J Med Genet. 2010;47(7):476–485. - PubMed
-
- Konradsen TR, Zetterstrom C. A descriptive study of ocular characteristics in Marfan syndrome. Acta Ophthalmol. 2013;91(8):751–755. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
