

DPPX antibody-associated encephalitis: Main syndrome and antibody effects
- PMID: 28258082
- PMCID: PMC5379928
- DOI: 10.1212/WNL.0000000000003796
DPPX antibody-associated encephalitis: Main syndrome and antibody effects
Abstract
Objective: To report the main syndrome of dipeptidyl-peptidase-like protein 6 (DPPX) antibody-associated encephalitis, immunoglobulin G (IgG) subclass, and the antibody effects on DPPX/Kv4.2 potassium channels.
Methods: A retrospective analysis of new patients and cases reported since 2013 was performed. IgG subclass and effects of antibodies on cultured neurons were determined with described techniques.
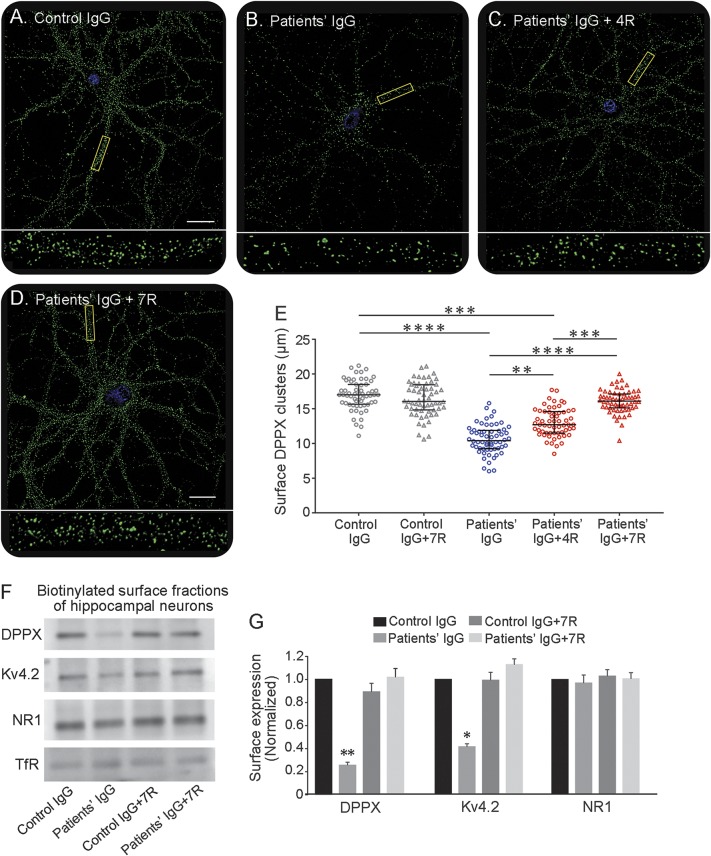
Results: Nine new patients were identified (median age 57 years, range 36-69 years). All developed severe prodromal weight loss or diarrhea followed by cognitive dysfunction (9), memory deficits (5), CNS hyperexcitability (8; hyperekplexia, myoclonus, tremor, or seizures), or brainstem or cerebellar dysfunction (7). The peak of the disease was reached 8 months (range 1-54 months) after onset. All patients had both IgG4 and IgG1 DPPX antibodies. In cultured neurons, the antibodies caused a decrease of DPPX clusters and Kv4.2 protein that was reversible on removal of the antibodies. Considering the current series and previously reported cases (total 39), 67% developed the triad: weight loss (median 20 kg; range 8-53 kg)/gastrointestinal symptoms, cognitive-mental dysfunction, and CNS hyperexcitability. Outcome was available from 35 patients (8 not treated with immunotherapy): 60% had substantial or moderate improvement, 23% had no improvement (most of them not treated), and 17% died. Relapses occurred in 8 of 35 patients (23%) and were responsive to immunotherapy.
Conclusions: DPPX antibodies are predominantly IgG1 and IgG4 and associate with cognitive-mental deficits and symptoms of CNS hyperexcitability that are usually preceded by diarrhea, other gastrointestinal symptoms, and weight loss. The disorder is responsive to immunotherapy, and this is supported by the reversibility of the antibody effects in cultured neurons.
© 2017 American Academy of Neurology.
Figures

References
-
- Balint B, Jarius S, Nagel S, et al. Progressive encephalomyelitis with rigidity and myoclonus: a new variant with DPPX antibodies. Neurology 2014;82:1521–1528. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical