

Restrictive versus liberal fluid therapy in major abdominal surgery (RELIEF): rationale and design for a multicentre randomised trial
- PMID: 28259855
- PMCID: PMC5353290
- DOI: 10.1136/bmjopen-2016-015358
Restrictive versus liberal fluid therapy in major abdominal surgery (RELIEF): rationale and design for a multicentre randomised trial
Abstract
Introduction: The optimal intravenous fluid regimen for patients undergoing major abdominal surgery is unclear. However, results from many small studies suggest a restrictive regimen may lead to better outcomes. A large, definitive clinical trial evaluating perioperative fluid replacement in major abdominal surgery, therefore, is required.
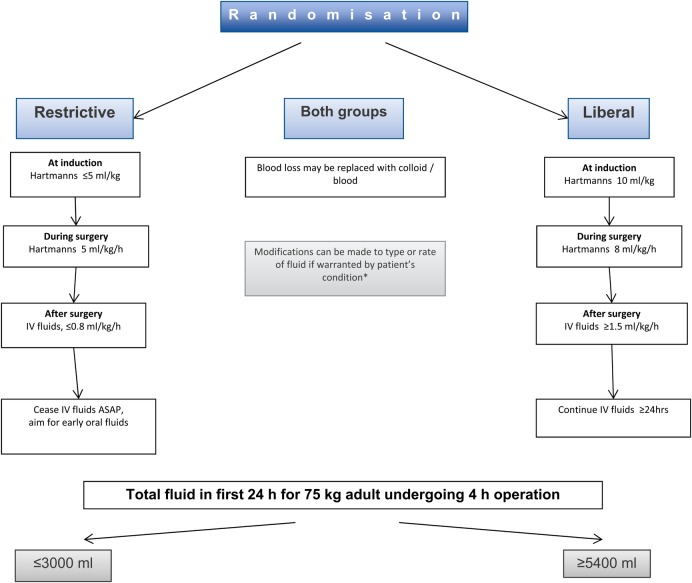
Methods/analysis: We designed a pragmatic, multicentre, randomised, controlled trial (the RELIEF trial). A total of 3000 patients were enrolled in this study and randomly allocated to a restrictive or liberal fluid regimen in a 1:1 ratio, stratified by centre and planned critical care admission. The expected fluid volumes in the first 24 hour from the start of surgery in restrictive and liberal groups were ≤3.0 L and ≥5.4 L, respectively. Patient enrolment is complete, and follow-up for the primary end point is ongoing. The primary outcome is disability-free survival at 1 year after surgery, with disability defined as a persistent (at least 6 months) reduction in functional status using the 12-item version of the World Health Organisation Disability Assessment Schedule.
Ethics/dissemination: The RELIEF trial has been approved by the responsible ethics committees of all participating sites. Participant recruitment began in March 2013 and was completed in August 2016, and 1-year follow-up will conclude in August 2017. Publication of the results of the RELIEF trial is anticipated in early 2018.
Trial registration number: ClinicalTrials.gov identifier NCT01424150.
Keywords: ANAESTHETICS; INTENSIVE & CRITICAL CARE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures
Comment in
-
Abdomeneingriffe: Liberale versus restriktive perioperative Flüssigkeitszufuhr.Aktuelle Urol. 2019 Jul;50(3):226-228. doi: 10.1055/a-0645-7571. Epub 2019 Jul 23. Aktuelle Urol. 2019. PMID: 31342483 German. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical