Review
doi: 10.14366/usg.17001.
Epub 2017 Jan 30.
Ultrasonography of the lower extremity veins: anatomy and basic approach
Affiliations
- PMID: 28260355
- PMCID: PMC5381851
- DOI: 10.14366/usg.17001
Item in Clipboard
Review
Ultrasonography of the lower extremity veins: anatomy and basic approach
Ultrasonography.
2017 Apr.
Abstract
Ultrasonography is an imaging modality widely used to evaluate venous diseases of the lower extremities. It is important to understand the normal venous anatomy of the lower extremities, which has deep, superficial, and perforating venous components, in order to determine the pathophysiology of venous disease. This review provides a basic description of the anatomy of the lower extremity veins and useful techniques for approaching each vein via ultrasonography.
Keywords: Anatomy; Lower extremity; Ultrasonography; Vein.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

The venous system of the lower extremities is classified into three groups: deep veins, which lie beneath the muscular fascia (dotted lines); superficial veins, which are situated above the muscular fascia; and perforating veins, which penetrate the muscular fascia and connect the superficial and deep veins. Note the deep vein (femoral vein, arrows), superficial vein (great saphenous vein, open arrows), and perforating vein (femoral canal perforator, arrowheads) of the thigh.
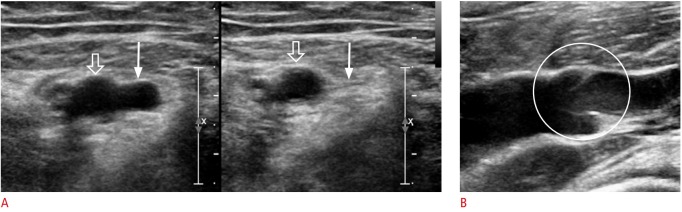
A. In contrast to arteries (open arrows), veins (arrows) have a weaker muscular layer with less elastic walls, and therefore completely collapse when compressed by the transducer. B. Veins contain valves that play an important role in preventing venous reflux.
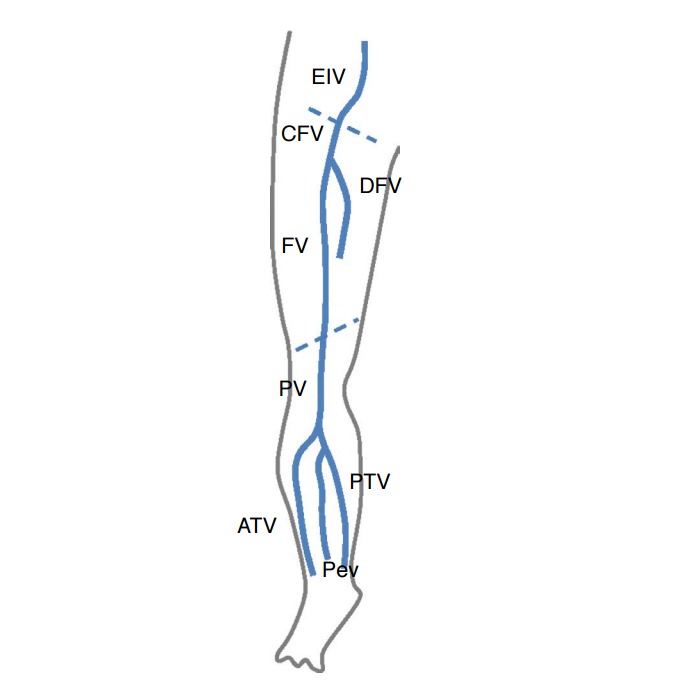
Although lower extremity veins form a continuous structure, they are named individually according to their closest anatomic landmark. The inguinal ligament (upper dotted line) is the anatomic landmark between the external iliac and common femoral veins, and the adductor hiatus (lower dotted line) is the anatomic landmark between the femoral and popliteal veins. EIV, external iliac vein; CFV, common femoral vein; FV, femoral vein; DFV, deep femoral vein; PV, popliteal vein; ATV, anterior tibial vein; PTV, posterior tibial vein; PeV, peroneal vein.
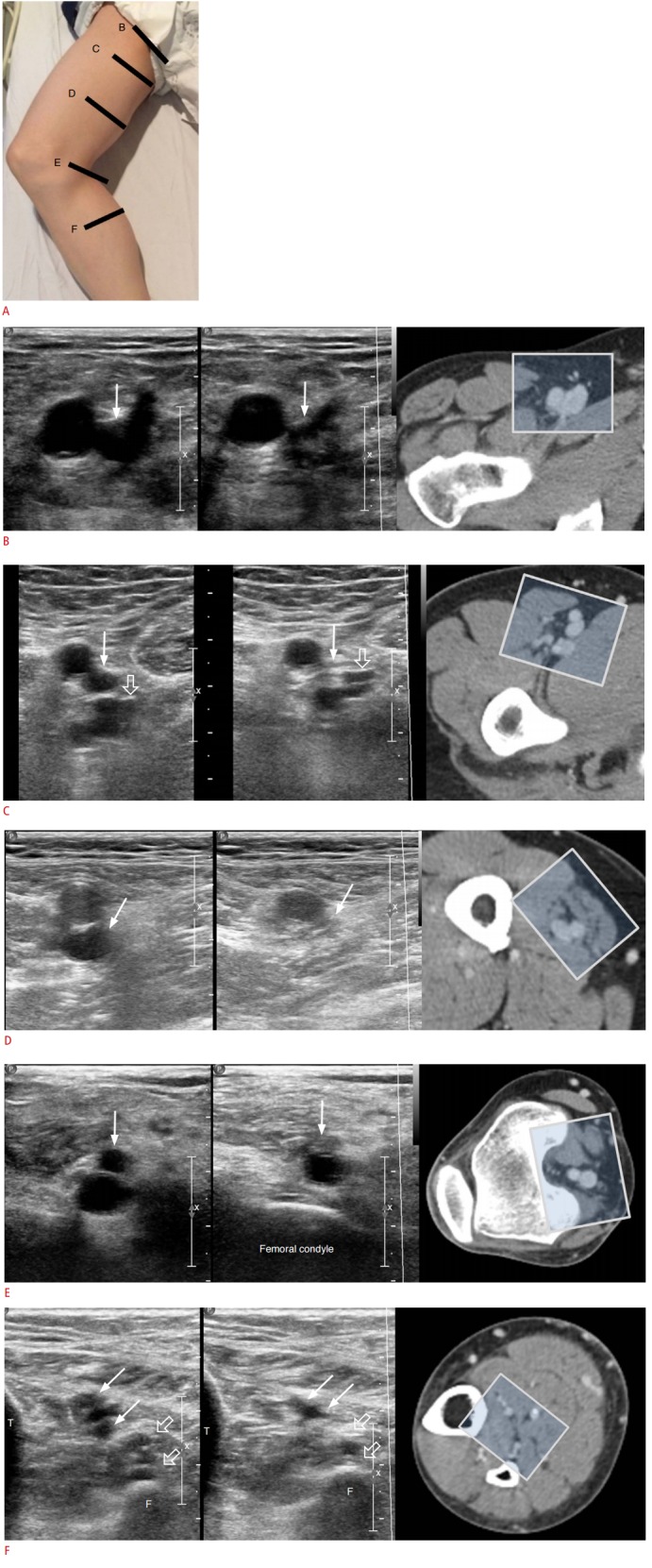
A. Patient position and schematic representation of the transducer locations are shown here (B, C, D, E, and F). B. The common femoral vein is seen at the level of the inguinal ligament on the medial side of the common femoral artery, which is round and pulsatile. The vein collapses upon compression (arrows). C. Upon following the common femoral vein downward, it bifurcates into the deep femoral vein (open arrows) and the femoral vein (arrows).
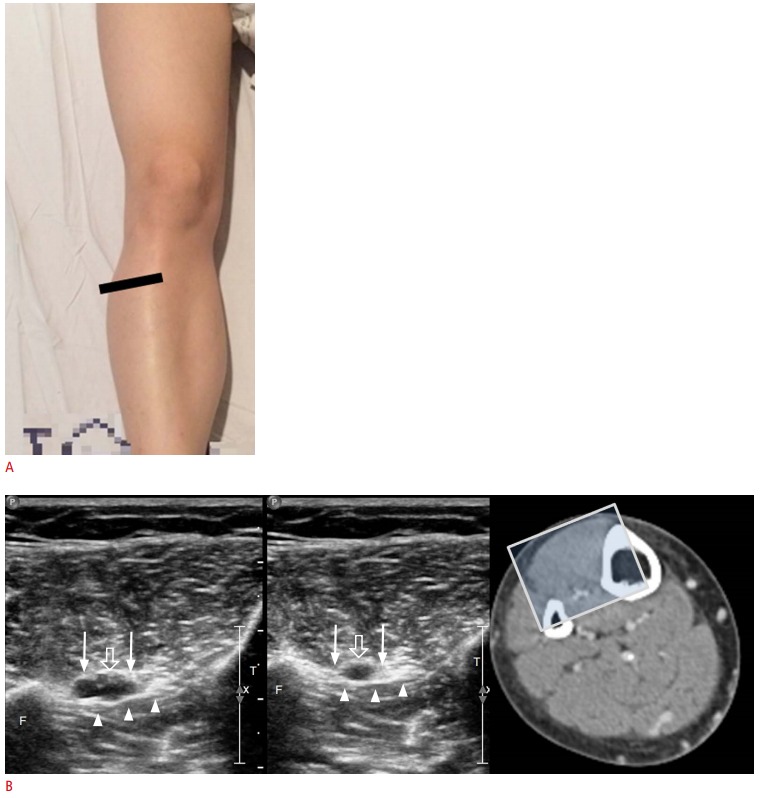
A. Stretching of the patient’s leg permits approach to the anterior tibial vein from the anterior side. B. Above the interosseous membrane (arrowheads) between the tibia (T) and the fibula (F), the anterior tibial vein (arrows) and artery (open arrows) are visible. The sonic window is demonstrated through computed tomography venography.
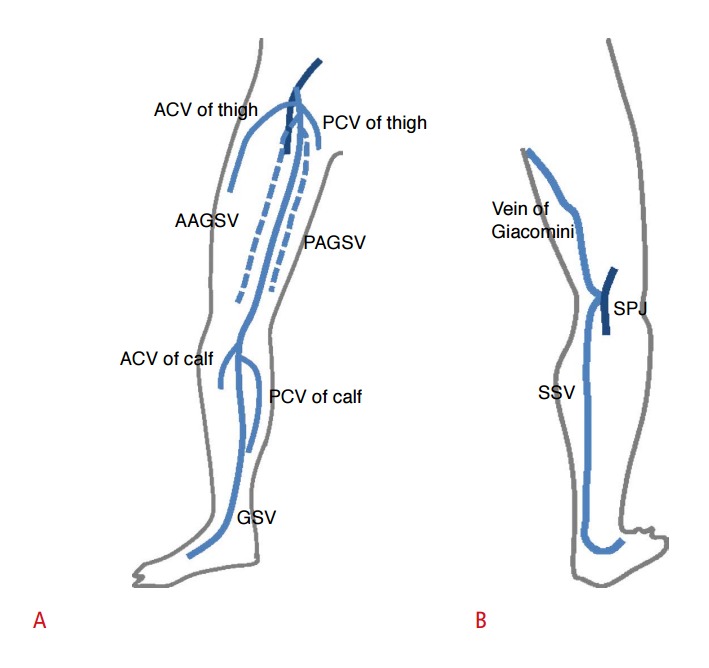
A. The great saphenous vein (GSV) arises from the medial aspect of the dorsal pedal venous arch, ascends anteriorly to the medial malleolus, passes posteromedially to the knee, and ascends medially in the thigh to join the common femoral vein through the saphenofemoral junction. Tributaries of the GSV are named according to their course. A tributary parallel to the GSV is called an accessory GSV. A tributary that courses obliquely is called a circumflex vein. ACV, anterior circumflex vein; PCV, posterior circumflex vein; AAGSV, anterior accessory great saphenous vein; PAGSV, posterior accessory great saphenous vein. B. The small saphenous vein (SSV) arises from the dorsal pedal arch and ascends along the middle of the calf and ends in the popliteal vein through the saphenopopliteal junction (SPJ). Before it penetrates the muscular fascia, the SSV may branch out a cranial extension, known as the vein of Giacomini, which goes upward to join the GSV.
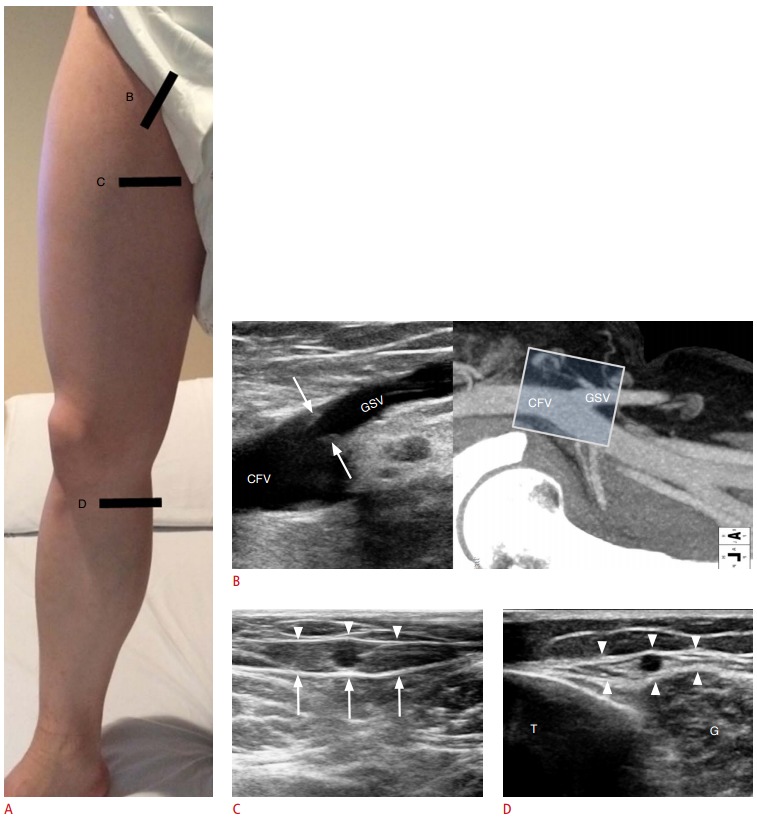
A. Patient position (standing) and schematic representation of the transducer locations are shown here. B. Longitudinal view of the saphenofemoral junction and the corresponding sonic window in computed tomography venography based on transducer location are demonstrated. In most cases, a terminal valve (arrows) near the saphenofemoral junction prevents backward flow into the great saphenous vein. CFV, common femoral vein. C. Examination of the GSV shows the echogenic fascia surrounding the GSV, which is bordered deeply by the muscular fascia (arrows) and superficially by the saphenous fascia (arrowheads). This saphenous compartment is readily visualized on ultrasonography and is described as having an “Egyptian eye” appearance. D. Transverse ultrasonography examination at the level of the knee shows the saphenous compartment (arrowheads) overlying the tibia (T) and the muscle fascia of the medial gastrocnemius (G).
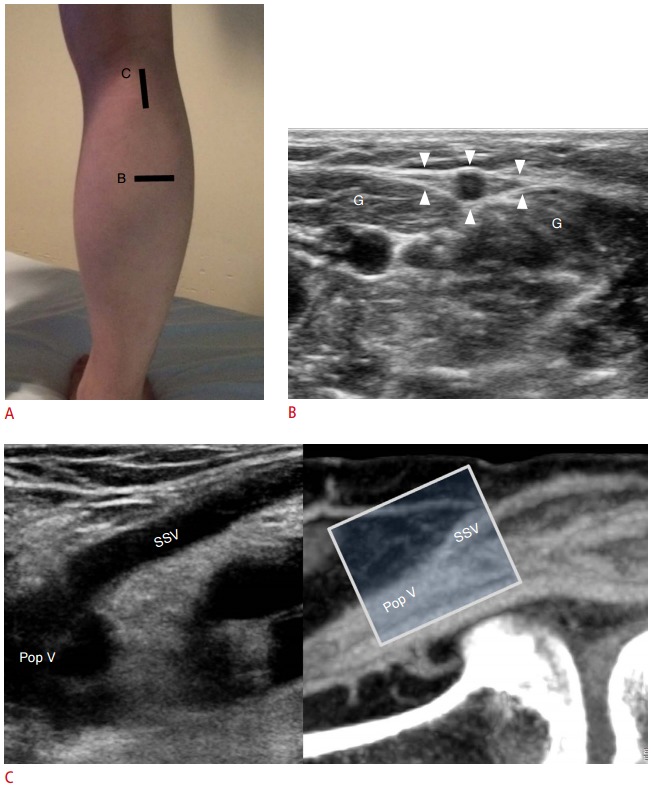
A. Patient position and schematic representation of the transducer locations are shown here. B. In the transverse view of the posterior calf, the SSV is seen in the middle of the gastrocnemius (G) belly in the fascial trunk (arrowheads). C. Longitudinal ultrasound view and the corresponding sonic window in computed tomography venography based on transducer location are demonstrated. The SSV joins the popliteal vein (Pop V) through the saphenopopliteal junction. However, many variations are noted in this region, and the saphenopopliteal junction can be absent or hypoplastic.
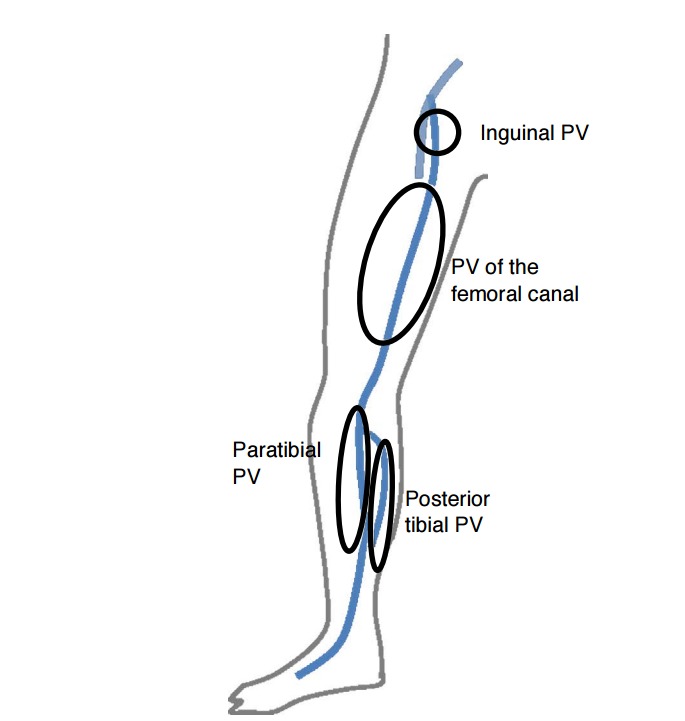
The PV of the medial leg includes the paratibial PV and the posterior tibial PV. The medial thigh perforator includes the PV of the femoral canal and the inguinal PV.
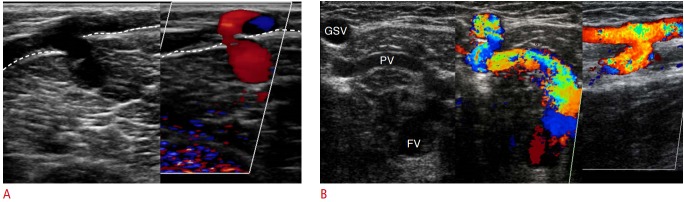
A. A dilated paratibial perforating vein in the calf is shown here, which penetrates the muscular fascia (dotted lines). B. A dilated PV of the femoral canal is shown here, which connects the great saphenous vein (GSV) and the femoral vein (FV). Venous reflux from the deep to the superficial vein is seen on transverse and longitudinal views of Doppler ultrasonography.
References
-
- Guideline developed in collaboration with the American College of Radiology. Society of Pediatric Radiology. Society of Radiologists in Ultrasound AIUM practice guideline for the performance of peripheral venous ultrasound examinations. J Ultrasound Med. 2015;34:1–9. - PubMed
-
- Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs: UIP consensus document. Part I. Basic principles. Eur J Vasc Endovasc Surg. 2006;31:83–92. - PubMed
-
- AbuRahma AF, Bandyk D. Noninvasive vascular diagnosis: a practical guide to therapy. 3rd ed. New York: Springer; 2012.
-
- Oguzkurt L. Ultrasonographic anatomy of the lower extremity superficial veins. Diagn Interv Radiol. 2012;18:423–430. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources