

Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients
- PMID: 28261116
- PMCID: PMC5311041
- DOI: 10.3389/fpsyt.2017.00025
Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients
Abstract
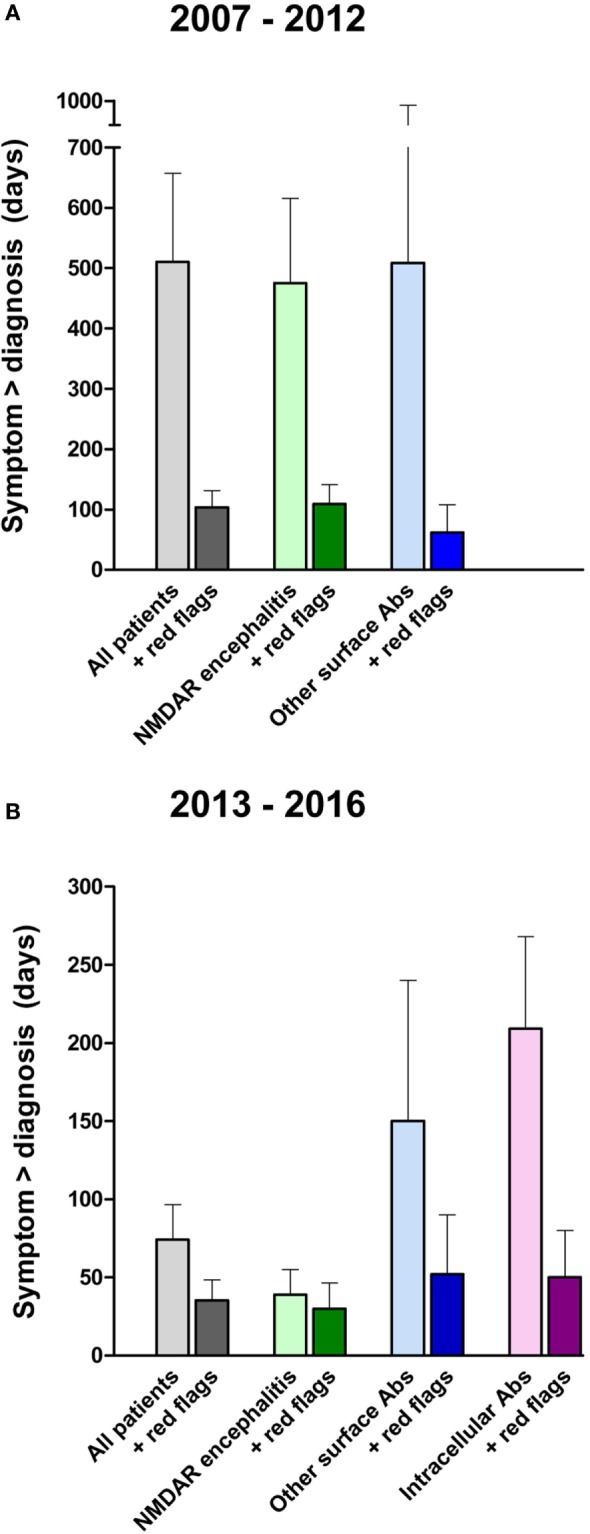
Autoimmune mechanisms causing diverse psychiatric symptoms are increasingly recognized and brought about a paradigm shift in neuropsychiatry. Identification of underlying antibodies against neuronal ion channels or receptors led to the speculation that a number of patients go misdiagnosed with a primary psychiatric disease. However, there is no clear consensus which clinical signs in psychiatric patients should prompt further investigations including measurement of anti-neuronal autoantibodies. We therefore aimed to analyze the presenting symptoms in patients with autoimmune encephalitis and the time between symptom onset and initiation of antibody diagnostics. For this, we recruited 100 patients from the Charité Center for Autoimmune Encephalitis between May and October 2016, including all types of autoimmune encephalitides. Psychiatric abnormalities were the most common clinical symptoms and were the presenting sign in 60%. One-third of patients were initially hospitalized in a psychiatric ward. All patients positive for antibodies against the N-methyl-d-aspartate receptor showed behavioral changes, hallucinations, memory deficits, catatonia, or delusions. Patients positive for antibodies against other cell surface or intracellular antigens were often hospitalized with a psychosomatic diagnosis. The time between occurrence of first symptoms and antibody testing was often alarmingly prolonged. In patients with symptom onset between 2013 and 2016, the mean delay was 74 days, in cases diagnosed between 2007 and 2012 even 483 days, suggesting though that increased awareness of this novel disease group helped to expedite proper diagnosis and treatment. By analyzing the medical records in detail, we identified clinical signs that may help to assist in earlier diagnosis, including seizures, catatonia, autonomic instability, or hyperkinesia. Indeed, reanalyzing the whole cohort using these "red flags" led to a 58% reduction of time between symptom onset and diagnosis. We conclude that the timely diagnosis of an autoimmune psychiatric disease can be facilitated by use of the described clinical warning signs, likely enabling earlier immunotherapy and better prognosis. Also, the threshold for cerebrospinal fluid analysis and autoantibody testing should be low.
Keywords: anti-neuronal autoantibodies; autoimmune encephalitis; cerebrospinal fluid analysis; immunotherapy; schizophreniform syndrome.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources