

Outcome of Laparoscopic Adrenalectomy in Obese Patients
- PMID: 28261359
- PMCID: PMC5327837
Outcome of Laparoscopic Adrenalectomy in Obese Patients
Abstract
Objectives: To compare early morbidity of obese and nonobese patients with minimally invasive adrenalectomies.
Method: Retrospective study of a prospectively maintained database, between June 2003 - December 2012, in a universitary affiliated tertiary hospital. Selection criteria: Minimally invasive adrenalectomy. Obese patients were defined as BMI over 30 kg/m2.
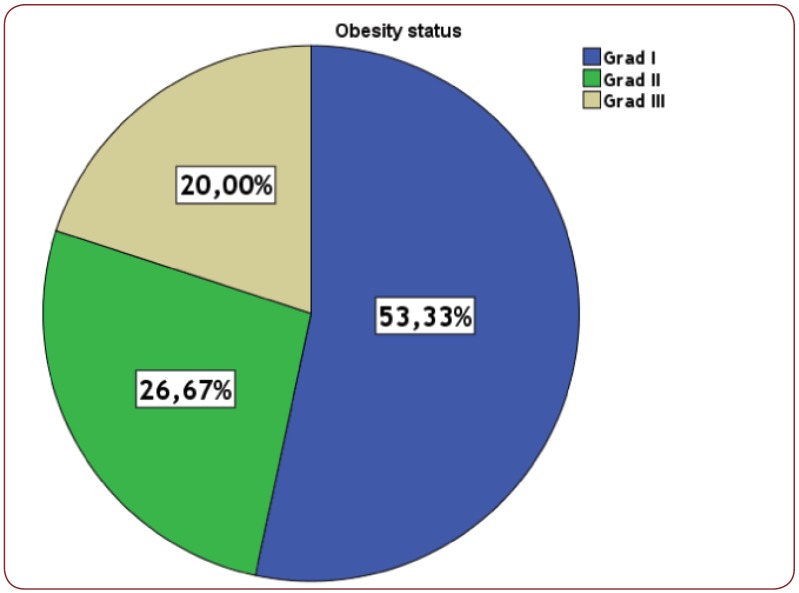
Results: From 205 patient with laparoscopic adrenalectomies we counted 30 obese patients (OG), 25 of them female and only 5 men with a median age of 54,20 years versus 47,94 years for nonobese group (NOG) (p=0.008). In OG were 15 right sided tumor, 11 on the left side and 4 bilateral all treated with transperitoneal antero-lateral approach. Median operating time was 92.20 minutes for OG versus 91.13 minutes for NOG (p=0.924). In OG, 5 patients had previous abdominal surgeries and we counted 4 conversion to open surgery, 2 postoperative complications (6.6%) and no mortality. All OG patients have diverse comorbidities, 50% of them more then 3. Median specimen size was 5.92 cm for OG versus 4.85 cm for NOG (p=0.057). The histology of OG was: adenoma 11 cases, hiperplasia 13 cases and pheochromocytoma 6. In NOG we had: postoperative hospital stay was 6.57 days in OG versus 4.11 days in NOG (p=0.009).
Conclusions: Although obese patients had a higher rate for early morbidities, the minimally invasive approach has particular benefits for them. Although postoperative hospital stay was significantly longer, we believe that advantages of minimal invasive surgery for obese patients remains valid even in a BMI over 30.
Figures








Similar articles
-
Results of femoral intramedullary nailing in patients who are obese versus those who are not obese: a prospective multicenter comparison study.J Orthop Trauma. 2007 Sep;21(8):523-9. doi: 10.1097/BOT.0b013e31813347ac. J Orthop Trauma. 2007. PMID: 17805018 Clinical Trial.
-
Impact of obesity on short-term results of laparoscopic rectal cancer resection.Surg Endosc. 2009 Jul;23(7):1460-4. doi: 10.1007/s00464-008-0266-5. Epub 2008 Dec 31. Surg Endosc. 2009. PMID: 19116737
-
Transperitoneal laparoscopic adrenalectomy in children.JSLS. 2014 Jul-Sep;18(3):e2014.00388. doi: 10.4293/JSLS.2014.00388. JSLS. 2014. PMID: 25392674 Free PMC article.
-
Comparison of laparoscopic transabdominal lateral versus posterior retroperitoneal adrenalectomy.Surgery. 2009 Oct;146(4):621-5; discussion 625-6. doi: 10.1016/j.surg.2009.06.057. Surgery. 2009. PMID: 19789020
-
Initial experience with laparoscopic adrenal surgery in children: is endoscopic surgery recommended and safe for the treatment of adrenocortical neoplasms?Pediatr Med Chir. 2004 Nov-Dec;26(6):450-9. Pediatr Med Chir. 2004. PMID: 16363772 Review.
Cited by
-
A comprehensive review and meta-analysis comparing robot-assisted and laparoscopic adrenalectomy in individuals with obesity.J Robot Surg. 2024 Aug 28;18(1):331. doi: 10.1007/s11701-024-02084-5. J Robot Surg. 2024. PMID: 39196416 Review.
-
Peri- and postoperative outcomes of laparoscopic adrenalectomy in nonobese versus obese patients: a systematic review and meta-analysis.Wideochir Inne Tech Maloinwazyjne. 2022 Sep;17(3):430-440. doi: 10.5114/wiitm.2022.116407. Epub 2022 May 19. Wideochir Inne Tech Maloinwazyjne. 2022. PMID: 36187061 Free PMC article. Review.
-
Body mass index and outcomes of patients with laparoscopic adrenalectomy: a systematic review and meta-analysis protocol.BMJ Open. 2019 Jun 5;9(6):e028579. doi: 10.1136/bmjopen-2018-028579. BMJ Open. 2019. PMID: 31171554 Free PMC article.
-
Laparoscopic versus robotic adrenalectomy in severely obese patients.Surg Endosc. 2023 Feb;37(2):1107-1113. doi: 10.1007/s00464-022-09594-z. Epub 2022 Sep 19. Surg Endosc. 2023. PMID: 36123544
-
The effect of obesity on the outcomes of laparoscopic adrenal surgery in patients with Cushing syndrome.Ann Surg Treat Res. 2024 Aug;107(2):100-107. doi: 10.4174/astr.2024.107.2.100. Epub 2024 Jul 30. Ann Surg Treat Res. 2024. PMID: 39139828 Free PMC article.
References
-
- Gagner M, Lacroix A, Bolte E – - Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N Engl J Med. 1992;327:1033. - PubMed
-
- Higashihara E, Tanaka Y, Horie S, et al. - [A case report of laparoscopic adrenalectomy]. Nihon Hinyokika Gakkai zasshi The japanese journal of urology. 1992;83:1130–3. - PubMed
-
- Cheah WK, Clark OH, Horn JK, et al. - Laparoscopic adrenalectomy for pheochromocytoma. World J Surg. 2002;26:1048–51. - PubMed
-
- Mitchell JC, Parangi S - Laparoscopic adrenalectomy for pheochromocytoma. Curr Surg. 2003;2601:561–6. - PubMed
-
- Kalady MF, McKinlay R, Olson JA, et al. - Laparoscopic adrenalectomy for pheochromocytoma. A comparison to aldosteronoma and incidentaloma. Surg Endosc. 2004;18:621–5. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous