

Integrated Approaches for the Management of Staple Line Leaks following Sleeve Gastrectomy
- PMID: 28261497
- PMCID: PMC5312046
- DOI: 10.1155/2017/4703236
Integrated Approaches for the Management of Staple Line Leaks following Sleeve Gastrectomy
Abstract
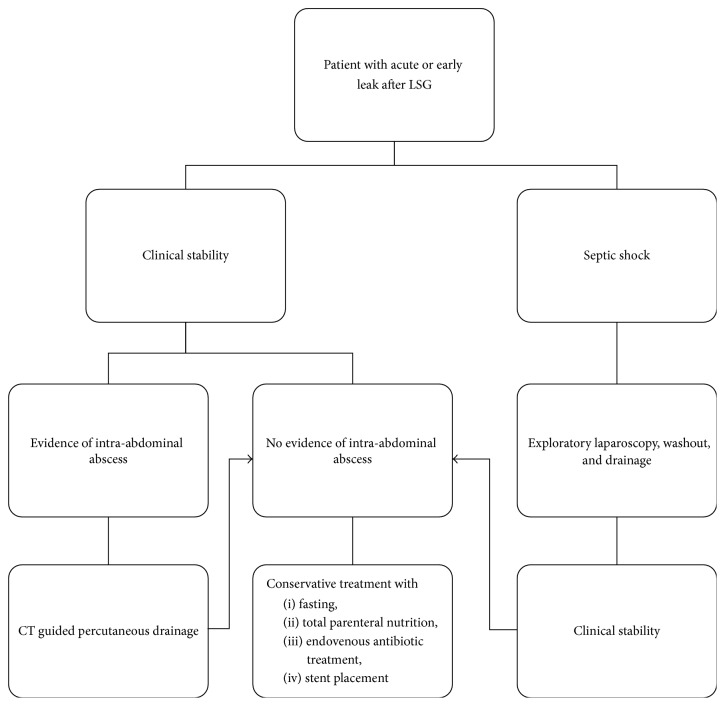
Introduction. Aim of the study was trying to draw a final flow chart for the management of gastric leaks after laparoscopic sleeve gastrectomy, based on the review of our cases over 10 years' experience. Material and Methods. We retrospectively reviewed all patients who underwent LSG as a primary operation at the Bariatric Unit of Tor Vergata University Hospital in Rome from 2007 to 2015. Results. Patients included in the study were 418. There were 6 staple line leaks (1.44%). All patients with diagnosis of a leak were initially discharged home in good clinical conditions and then returned to A&E because of the complication. The mean interval between surgery and readmission for leak was 13,4 days (range 6-34 days, SD ± 11.85). We recorded one death (16.67%) due to sepsis. The remaining five cases were successfully treated with a mean healing time of the gastric leak of 55,5 days (range 26-83 days; SD ± 25.44). Conclusion. Choosing the proper treatment depends on clinical stability and on the presence or not of collected abscess. Our treatment protocol showed being associated with low complication rate and minor discomfort to the patients, reducing the need for more invasive procedures.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures
Similar articles
-
Management of staple line leaks following sleeve gastrectomy.Surg Obes Relat Dis. 2015 Jan-Feb;11(1):54-9. doi: 10.1016/j.soard.2014.07.005. Epub 2014 Jul 10. Surg Obes Relat Dis. 2015. PMID: 25547056
-
Nonsurgical treatment of staple line leaks after laparoscopic sleeve gastrectomy.Obes Surg. 2009 Jul;19(7):821-6. doi: 10.1007/s11695-009-9840-8. Epub 2009 Apr 21. Obes Surg. 2009. PMID: 19381737
-
The utility of radiological upper gastrointestinal series and clinical indicators in detecting leaks after laparoscopic sleeve gastrectomy: a case-controlled study.Surg Endosc. 2016 Jun;30(6):2266-75. doi: 10.1007/s00464-015-4516-z. Epub 2015 Sep 28. Surg Endosc. 2016. PMID: 26416376
-
Reinforcement does not necessarily reduce the rate of staple line leaks after sleeve gastrectomy. A review of the literature and clinical experiences.Obes Surg. 2009 Feb;19(2):166-172. doi: 10.1007/s11695-008-9668-7. Epub 2008 Sep 16. Obes Surg. 2009. PMID: 18795383 Review.
-
A Narrative of Intraoperative Staple Line Leaks and Bleeds During Bariatric Surgery.Obes Surg. 2016 Jul;26(7):1601-6. doi: 10.1007/s11695-016-2177-1. Obes Surg. 2016. PMID: 27094877 Free PMC article. Review.
Cited by
-
Management of Staple Line Leaks Following Sleeve Gastrectomy-a Systematic Review.Obes Surg. 2019 Sep;29(9):2759-2772. doi: 10.1007/s11695-019-03896-3. Obes Surg. 2019. PMID: 31062278
-
Measuring Knowledge, Attitudes, and Barriers to Medication Adherence in Potential Bariatric Surgery Patients.Obes Surg. 2021 Sep;31(9):4045-4054. doi: 10.1007/s11695-021-05485-9. Epub 2021 Jul 2. Obes Surg. 2021. PMID: 34212345 Free PMC article.
-
Assessing psychopathology in bariatric surgery candidates: discriminant validity of the SCL-90-R and SCL-K-9 in a large sample of patients.Eat Weight Disord. 2021 Oct;26(7):2211-2218. doi: 10.1007/s40519-020-01068-2. Epub 2020 Nov 23. Eat Weight Disord. 2021. PMID: 33226607 Free PMC article.
-
Customized bariatric stents for sleeve gastrectomy leak: are they superior to conventional esophageal stents? A systematic review and proportion meta-analysis.Surg Endosc. 2021 Mar;35(3):1025-1038. doi: 10.1007/s00464-020-08147-6. Epub 2020 Nov 6. Surg Endosc. 2021. PMID: 33159298
-
Results of The Comparative Study of 200 Cases: One Anastomosis Gastric Bypass vs Roux-en-Y Gastric Bypass.Obes Surg. 2018 Sep;28(9):2597-2602. doi: 10.1007/s11695-018-3224-x. Obes Surg. 2018. PMID: 29713942
References
-
- NHLBI Obesity Education Initiative Expert Panel on the Identification. The Evidence Report. 98-4083. Bethesda, Md, USA: National Heart, Lung, and Blood Institute; 1998. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. https://www.ncbi.nlm.nih.gov/
-
- Perrone F., Bianciardi E., Benavoli D., et al. Gender influence on long-term weight loss and comorbidities after laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: a prospective study with a 5-year follow-up. Obesity Surgery. 2016;26(2):276–281. doi: 10.1007/s11695-015-1746-z. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
