

An Emergency Department Validation of the SEP-3 Sepsis and Septic Shock Definitions and Comparison With 1992 Consensus Definitions
- PMID: 28262318
- PMCID: PMC5792164
- DOI: 10.1016/j.annemergmed.2017.01.008
An Emergency Department Validation of the SEP-3 Sepsis and Septic Shock Definitions and Comparison With 1992 Consensus Definitions
Abstract
Study objective: The Third International Consensus Definitions Task Force (SEP-3) proposed revised criteria defining sepsis and septic shock. We seek to evaluate the performance of the SEP-3 definitions for prediction of inhospital mortality in an emergency department (ED) population and compare the performance of the SEP-3 definitions to that of the previous definitions.
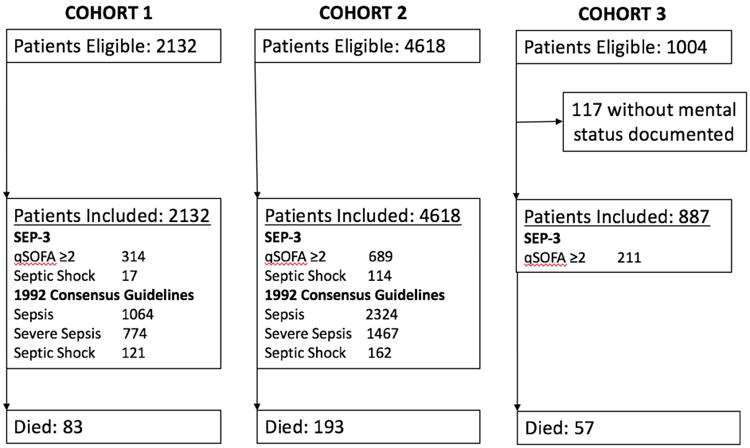
Methods: This was a secondary analysis of 3 prospectively collected, observational cohorts of infected ED subjects aged 18 years or older. The primary outcome was all-cause inhospital mortality. In accordance with the SEP-3 definitions, we calculated test characteristics of sepsis (quick Sequential Organ Failure Assessment [qSOFA] score ≥2) and septic shock (vasopressor dependence plus lactate level >2.0 mmol/L) for mortality and compared them to the original 1992 consensus definitions.
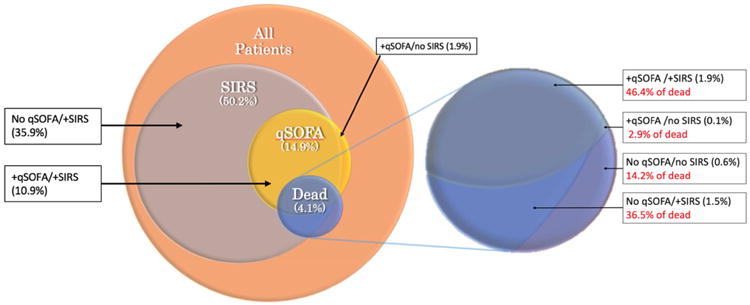
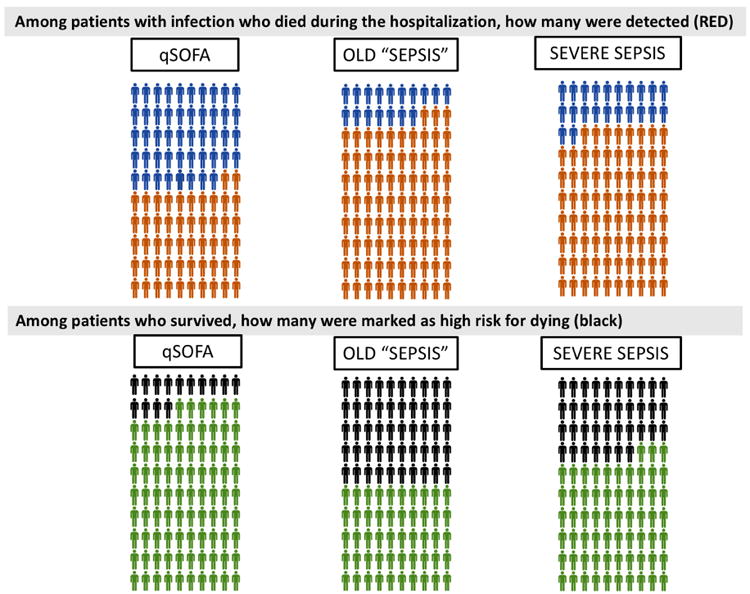
Results: We identified 7,754 ED patients with suspected infection overall; 117 had no documented mental status evaluation, leaving 7,637 patients included in the analysis. The mortality rate for the overall population was 4.4% (95% confidence interval [CI] 3.9% to 4.9%). The mortality rate for patients with qSOFA score greater than or equal to 2 was 14.2% (95% CI 12.2% to 16.2%), with a sensitivity of 52% (95% CI 46% to 57%) and specificity of 86% (95% CI 85% to 87%) to predict mortality. The original systemic inflammatory response syndrome-based 1992 consensus sepsis definition had a 6.8% (95% CI 6.0% to 7.7%) mortality rate, sensitivity of 83% (95% CI 79% to 87%), and specificity of 50% (95% CI 49% to 51%). The SEP-3 septic shock mortality was 23% (95% CI 16% to 30%), with a sensitivity of 12% (95% CI 11% to 13%) and specificity of 98.4% (95% CI 98.1% to 98.7%). The original 1992 septic shock definition had a 22% (95% CI 17% to 27%) mortality rate, sensitivity of 23% (95% CI 18% to 28%), and specificity of 96.6% (95% CI 96.2% to 97.0%).
Conclusion: Both the new SEP-3 and original sepsis definitions stratify ED patients at risk for mortality, albeit with differing performances. In terms of mortality prediction, the SEP-3 definitions had improved specificity, but at the cost of sensitivity. Use of either approach requires a clearly intended target: more sensitivity versus specificity.
Copyright © 2017 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Prognostic Accuracy of Quick Sequential Organ Failure Assessment Among Emergency Department Patients Admitted to an ICU.Ann Emerg Med. 2017 Oct;70(4):600-601. doi: 10.1016/j.annemergmed.2017.05.028. Ann Emerg Med. 2017. PMID: 28946985 No abstract available.
-
In reply.Ann Emerg Med. 2017 Oct;70(4):601. doi: 10.1016/j.annemergmed.2017.05.029. Ann Emerg Med. 2017. PMID: 28946987 No abstract available.
References
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–1655. - PubMed
-
- Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Critical Care Medicine. 2003;31(4):1250–1256. - PubMed
-
- Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. New England Journal of Medicine. 2015;372(17):1629–1638. - PubMed
-
- Gille-Johnson P, Hansson KE, Gårdlund B. Severe sepsis and systemic inflammatory response syndrome in emergency department patients with suspected severe infection. Scand J Infect Dis. 2013;45(3):186–193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
