

Intraoperative near-infrared fluorescence imaging targeting folate receptors identifies lung cancer in a large-animal model
- PMID: 28263385
- PMCID: PMC5341137
- DOI: 10.1002/cncr.30419
Intraoperative near-infrared fluorescence imaging targeting folate receptors identifies lung cancer in a large-animal model
Abstract
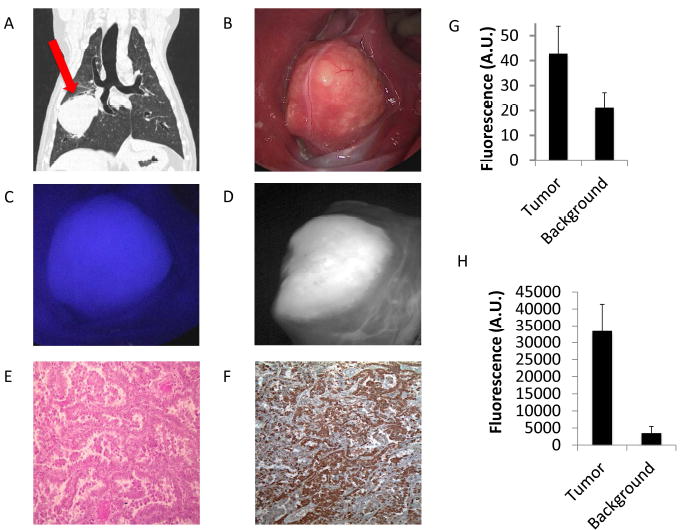
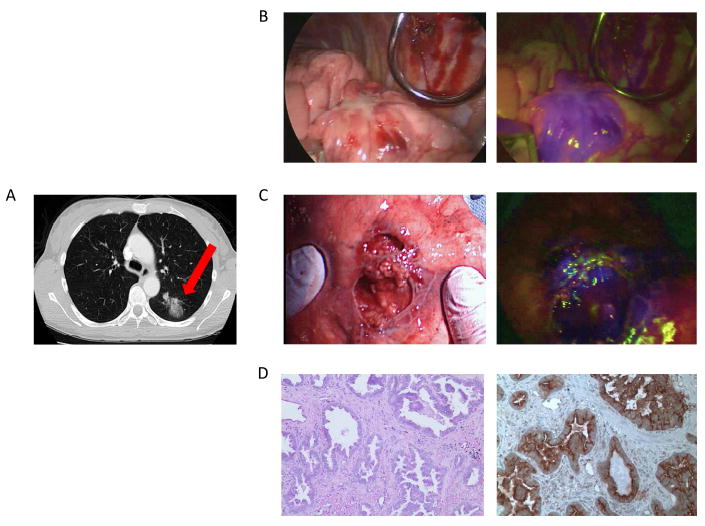
Background: Complete tumor resection is the most important predictor of patient survival with non-small cell lung cancer. Methods for intraoperative margin assessment after lung cancer excision are lacking. This study evaluated near-infrared (NIR) intraoperative imaging with a folate-targeted molecular contrast agent (OTL0038) for the localization of primary lung adenocarcinomas, lymph node sampling, and margin assessment.
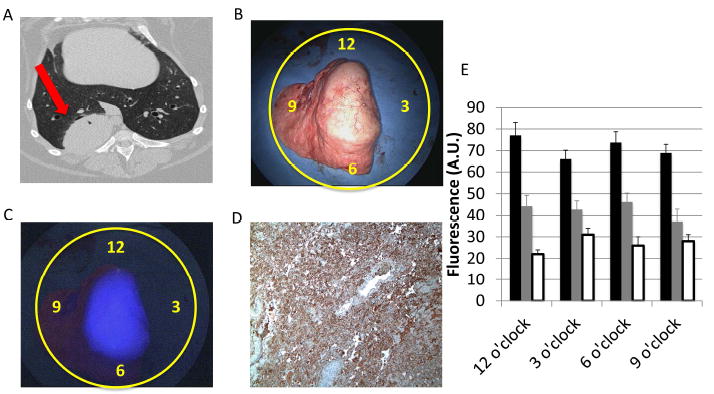
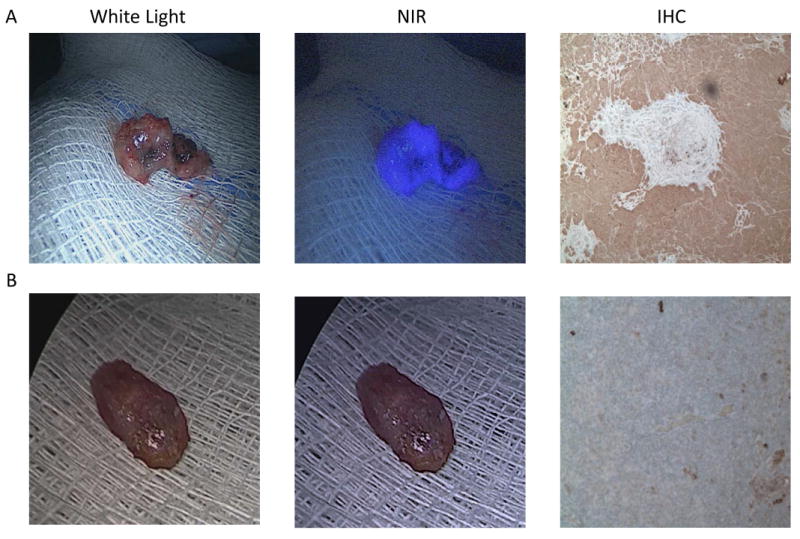
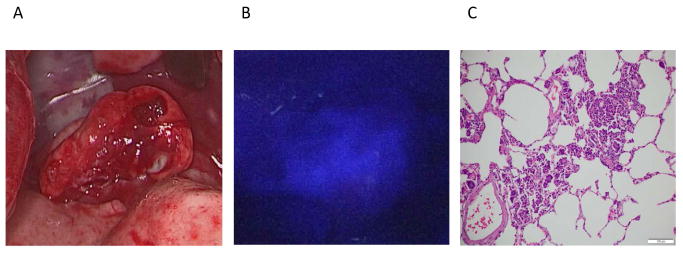
Methods: Ten dogs with lung cancer underwent either video-assisted thoracoscopic surgery or open thoracotomy and tumor excision after an intravenous injection of OTL0038. Lungs were imaged with an NIR imaging device both in vivo and ex vivo. The wound bed was re-imaged for retained fluorescence suspicious for positive tumor margins. The tumor signal-to-background ratio (SBR) was measured in all cases. Next, 3 human patients were enrolled in a proof-of-principle study. Tumor fluorescence was measured both in situ and ex vivo.
Results: All canine tumors fluoresced in situ (mean Fluoptics SBR, 5.2 [range, 2.7-8.1]; mean Karl Storz SBR 1.9 [range, 1.4-2.6]). In addition, the fluorescence was consistent with tumor margins on pathology. Three positive lymph nodes were discovered with NIR imaging. Also, a positive retained tumor margin was discovered upon NIR imaging of the wound bed. Human pulmonary adenocarcinomas were also fluorescent both in situ and ex vivo (mean SBR, > 2.0).
Conclusions: NIR imaging can identify lung cancer in a large-animal model. In addition, NIR imaging can discriminate lymph nodes harboring cancer cells and also bring attention to a positive tumor margin. In humans, pulmonary adenocarcinomas fluoresce after the injection of the targeted contrast agent. Cancer 2017;123:1051-60. © 2016 American Cancer Society.
Keywords: imaging; intraoperative; lung cancer; molecular; near-infrared.
© 2016 American Cancer Society.
Conflict of interest statement
Conflict of Interest: There are no conflict of interest disclosures for any author other than Dr. Low. Dr. Low reports grants and personal fees from On Target Laboratories. In addition, Dr. Low has a patent On Target Laboratories licensed.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 63:11–30. - PubMed
-
- Ramalingam SS, Owonikoko TK, Khuri FR. Lung cancer: New biological insights and recent therapeutic advances. CA Cancer J Clin. 2011;61:91–112. - PubMed
-
- Vallejo Ocana C, Garrido Lopez P, Muguruza Trueba I. Multidisciplinary approach in stage III non-small-cell lung cancer: standard of care and open questions. Clin Transl Oncol. 2011;13:629–635. - PubMed
-
- Sienel W, Stremmel C, Kirschbaum A, et al. Frequency of local recurrence following segmentectomy of stage IA non-small cell lung cancer is influenced by segment localisation and width of resection margins--implications for patient selection for segmentectomy. Eur J Cardiothorac Surg. 2007;31:522–527. discussion 527-528. - PubMed
-
- Kaiser LR, Fleshner P, Keller S, Martini N. Significance of extramucosal residual tumor at the bronchial resection margin. Ann Thorac Surg. 1989;47:265–269. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
