

Analysis of Machine Learning Techniques for Heart Failure Readmissions
- PMID: 28263938
- PMCID: PMC5459389
- DOI: 10.1161/CIRCOUTCOMES.116.003039
Analysis of Machine Learning Techniques for Heart Failure Readmissions
Abstract
Background: The current ability to predict readmissions in patients with heart failure is modest at best. It is unclear whether machine learning techniques that address higher dimensional, nonlinear relationships among variables would enhance prediction. We sought to compare the effectiveness of several machine learning algorithms for predicting readmissions.
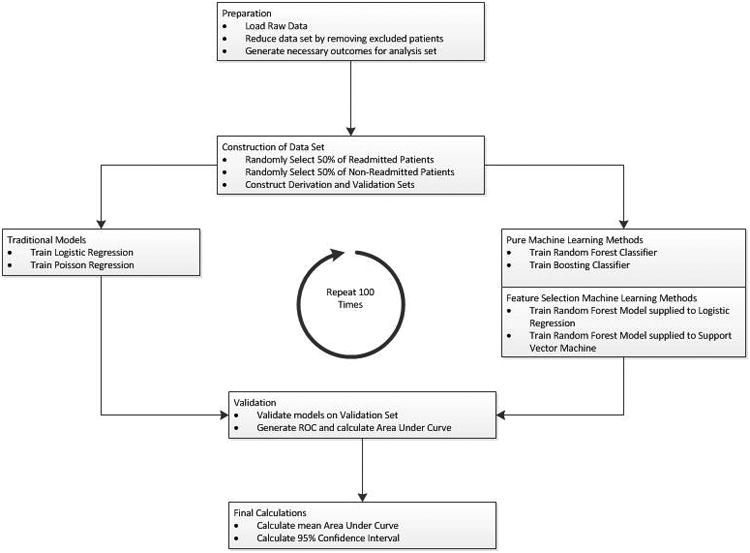
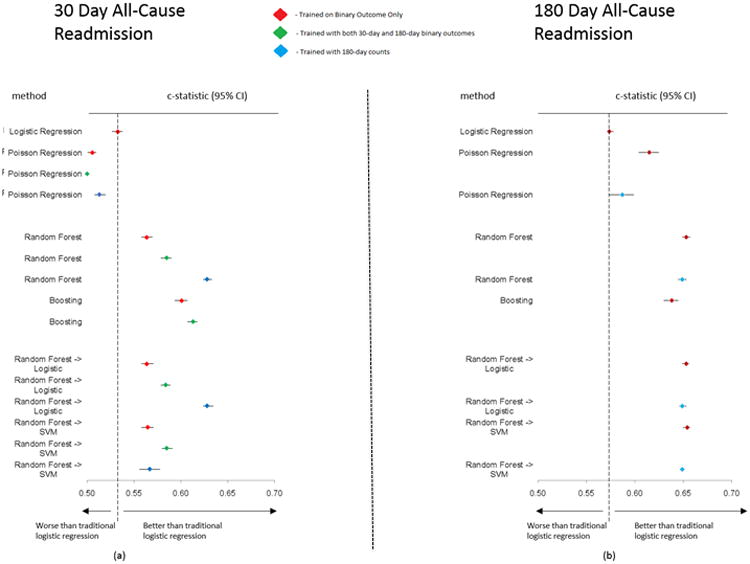
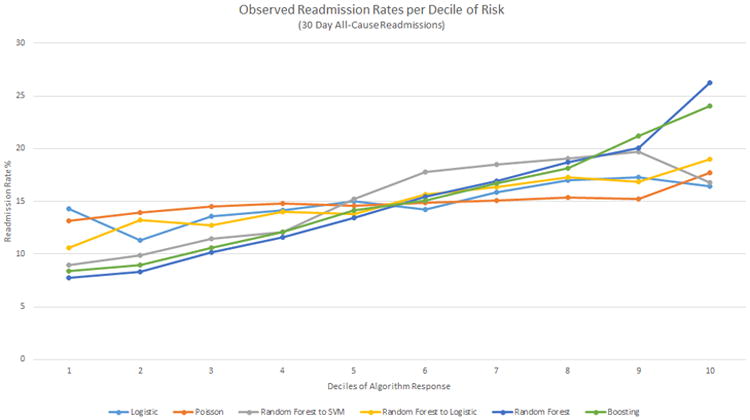
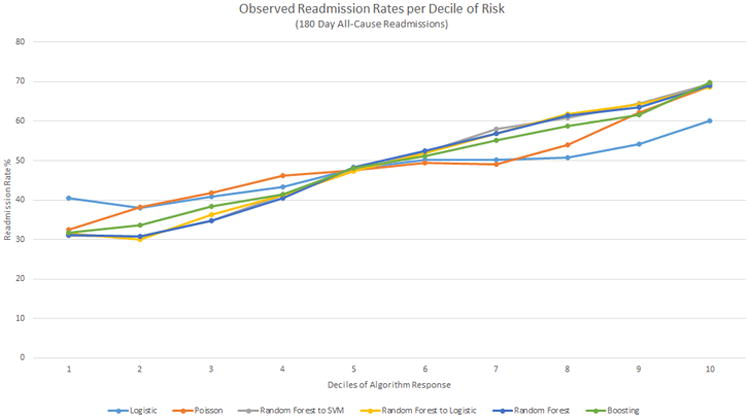
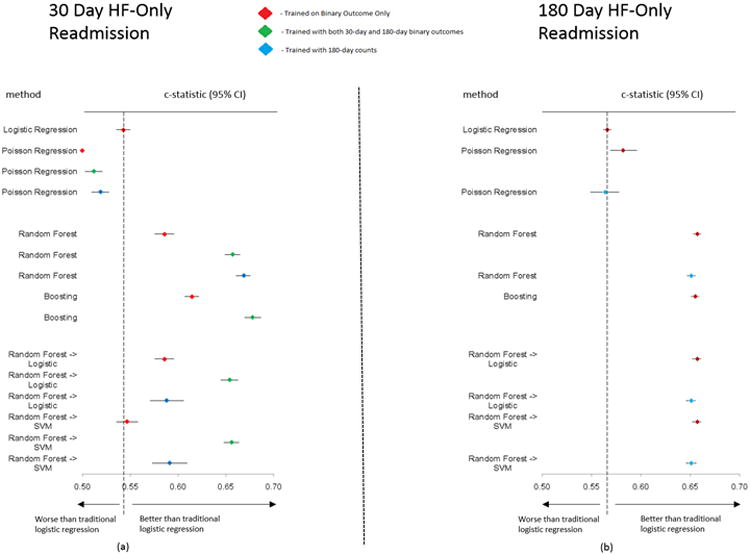
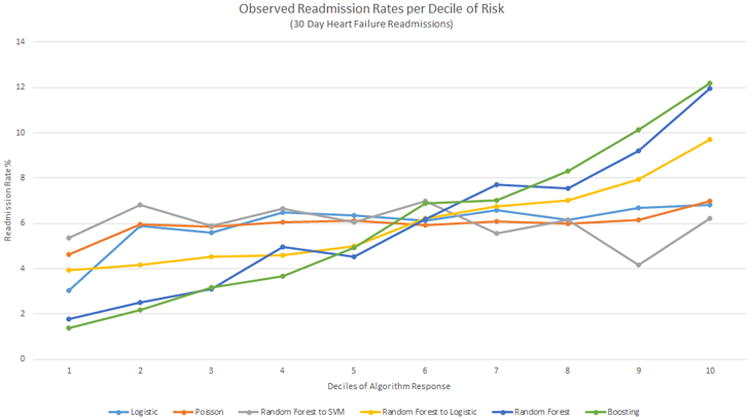
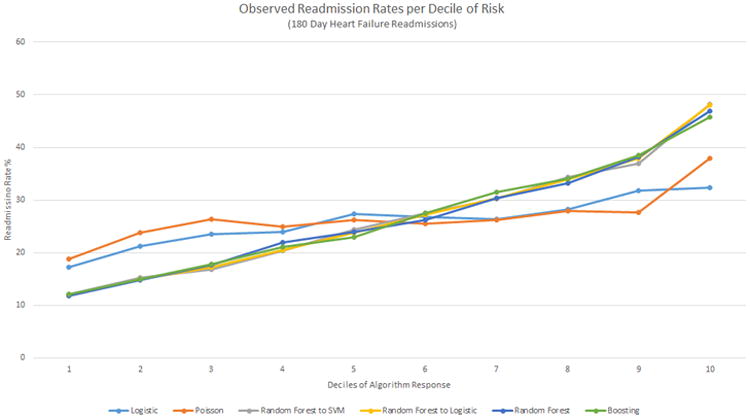
Methods and results: Using data from the Telemonitoring to Improve Heart Failure Outcomes trial, we compared the effectiveness of random forests, boosting, random forests combined hierarchically with support vector machines or logistic regression (LR), and Poisson regression against traditional LR to predict 30- and 180-day all-cause readmissions and readmissions because of heart failure. We randomly selected 50% of patients for a derivation set, and a validation set comprised the remaining patients, validated using 100 bootstrapped iterations. We compared C statistics for discrimination and distributions of observed outcomes in risk deciles for predictive range. In 30-day all-cause readmission prediction, the best performing machine learning model, random forests, provided a 17.8% improvement over LR (mean C statistics, 0.628 and 0.533, respectively). For readmissions because of heart failure, boosting improved the C statistic by 24.9% over LR (mean C statistic 0.678 and 0.543, respectively). For 30-day all-cause readmission, the observed readmission rates in the lowest and highest deciles of predicted risk with random forests (7.8% and 26.2%, respectively) showed a much wider separation than LR (14.2% and 16.4%, respectively).
Conclusions: Machine learning methods improved the prediction of readmission after hospitalization for heart failure compared with LR and provided the greatest predictive range in observed readmission rates.
Trial registration: ClinicalTrials.gov NCT00303212.
Keywords: computers; heart failure; machine learning; meta-analysis; patient readmission.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Kocher RP, Adashi EY. Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306:1794–1795. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
