

Early Detection of Heart Failure Using Electronic Health Records: Practical Implications for Time Before Diagnosis, Data Diversity, Data Quantity, and Data Density
- PMID: 28263940
- PMCID: PMC5341145
- DOI: 10.1161/CIRCOUTCOMES.116.002797
Early Detection of Heart Failure Using Electronic Health Records: Practical Implications for Time Before Diagnosis, Data Diversity, Data Quantity, and Data Density
Abstract
Background: Using electronic health records data to predict events and onset of diseases is increasingly common. Relatively little is known, although, about the tradeoffs between data requirements and model utility.
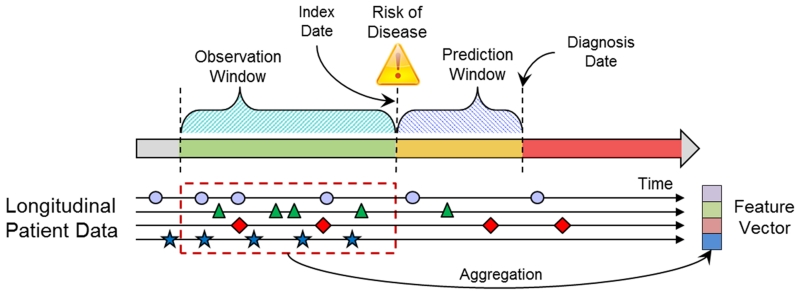
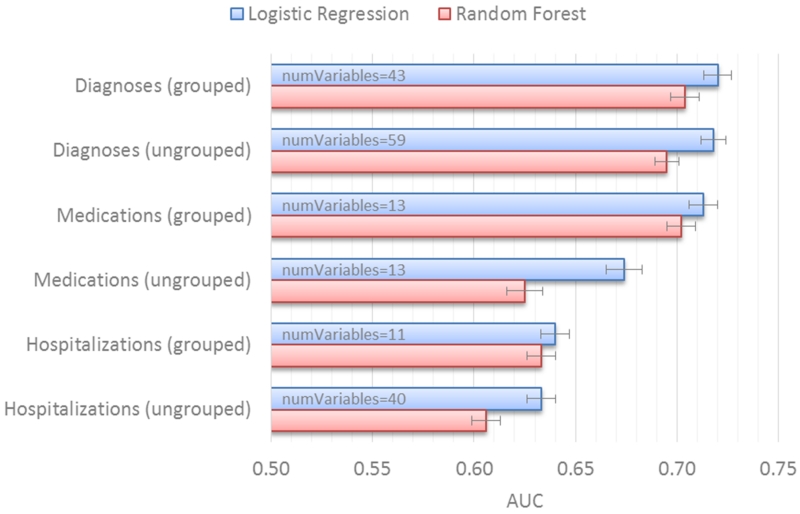
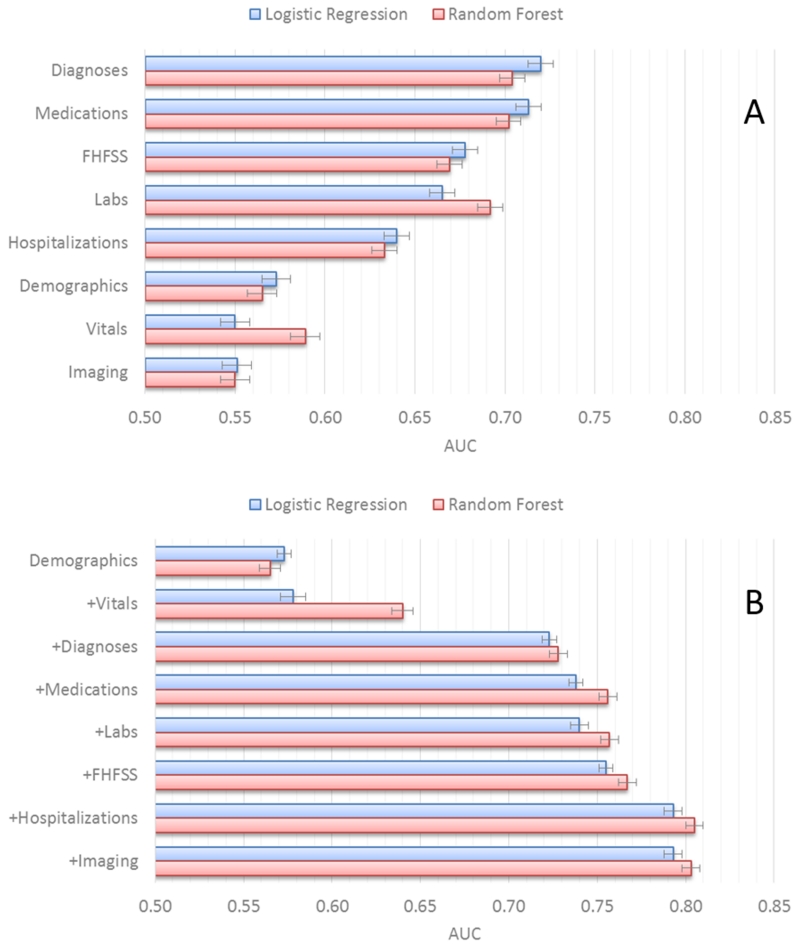
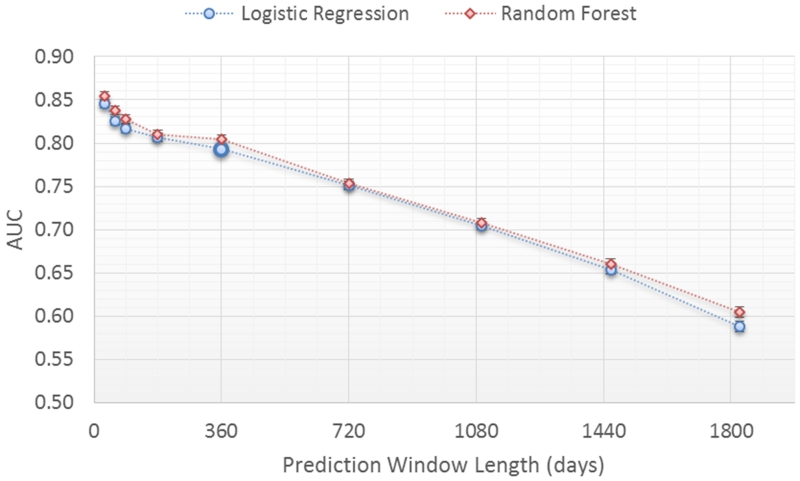
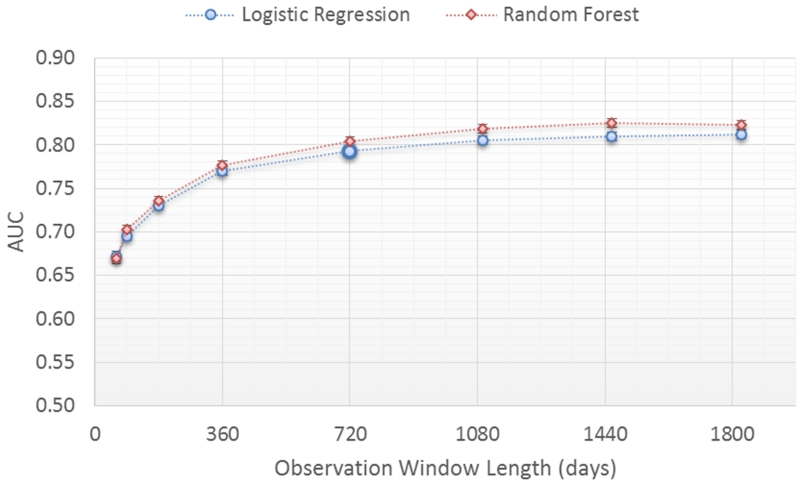
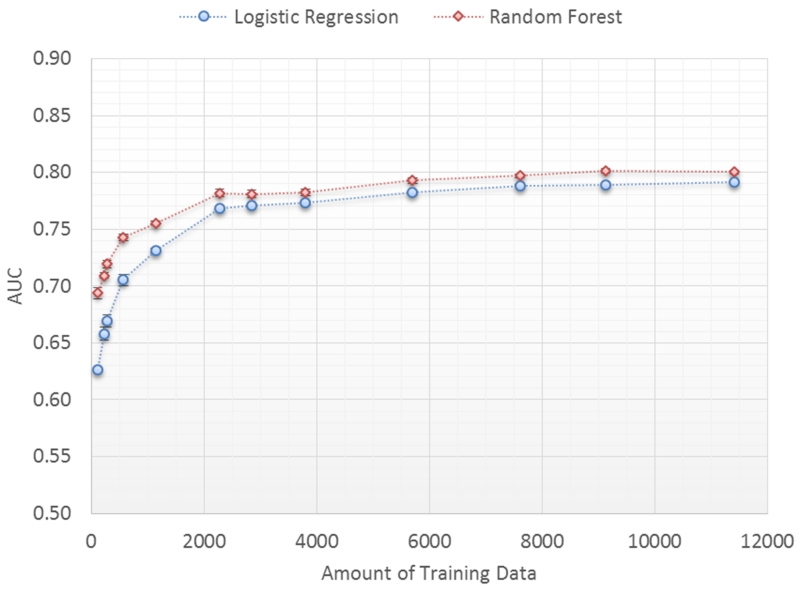
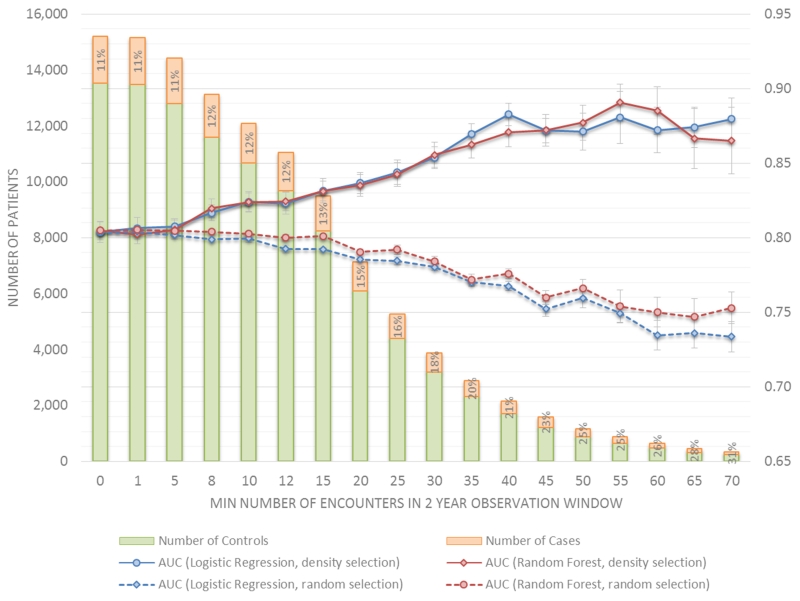
Methods and results: We examined the performance of machine learning models trained to detect prediagnostic heart failure in primary care patients using longitudinal electronic health records data. Model performance was assessed in relation to data requirements defined by the prediction window length (time before clinical diagnosis), the observation window length (duration of observation before prediction window), the number of different data domains (data diversity), the number of patient records in the training data set (data quantity), and the density of patient encounters (data density). A total of 1684 incident heart failure cases and 13 525 sex, age-category, and clinic matched controls were used for modeling. Model performance improved as (1) the prediction window length decreases, especially when <2 years; (2) the observation window length increases but then levels off after 2 years; (3) the training data set size increases but then levels off after 4000 patients; (4) more diverse data types are used, but, in order, the combination of diagnosis, medication order, and hospitalization data was most important; and (5) data were confined to patients who had ≥10 phone or face-to-face encounters in 2 years.
Conclusions: These empirical findings suggest possible guidelines for the minimum amount and type of data needed to train effective disease onset predictive models using longitudinal electronic health records data.
Keywords: diagnosis; electronic health records; heart failure; prevention and control; risk factors.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Learning About Machine Learning: The Promise and Pitfalls of Big Data and the Electronic Health Record.Circ Cardiovasc Qual Outcomes. 2016 Nov;9(6):618-620. doi: 10.1161/CIRCOUTCOMES.116.003308. Epub 2016 Nov 8. Circ Cardiovasc Qual Outcomes. 2016. PMID: 28263936 Free PMC article. No abstract available.
References
-
- Mozaffarian D, Benjamin E, Go A, Arnett D, Blaha M, Cushman M, Das S, deFerranti S, Després J-P, Fullerton H, Howard V, Huffman M, Isasi C, Jiménez M, Judd S, Kissela B, Lichtman J, Lisabeth L, Liu S, Mackey R, Magid D, McGuire D, Mohler E, Moy C, Muntner P, Mussolino M, Nasir K, Neumar R, Nichol G, Palaniappan L, Pandey D, Reeves M, Rodriguez C, Rosamond W, Sorlie P, Stein J, Towfighi A, Turan T, Virani S, Woo D, Yeh R, Turner M. Heart Disease and Stroke Statistics—2016 Update: A Report From the American Heart Association. Circulation. 2015;133:38–360. - PubMed
-
- Roger V, Weston S, Redfield M, Hellermann-Homan J, Killian J, Yawn B, Jacobsen S. Trends in heart failure incidence and survival in a community-based population. JAMA. 2014;292:344–350. - PubMed
-
- Murphy S, Xu J, Kochanek K. Deaths: final data for 2010. Natl Vital Stat Rep. 2013;61:1–117. - PubMed
-
- Vijayakrishnan R, Steinhubl S, Ng K, Sun J, Byrd R, Daar Z, Williams B, deFilippi C, Ebadollahi S, Stewart W. Prevalence of heart failure signs and symptoms in a large primary care population identified through the use of text and data mining of the electronic health record. J. Card. Fail. 2015;20:459–464. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
