

Reproducibility, reliability and validity of population-based administrative health data for the assessment of cancer non-related comorbidities
- PMID: 28263996
- PMCID: PMC5338773
- DOI: 10.1371/journal.pone.0172814
Reproducibility, reliability and validity of population-based administrative health data for the assessment of cancer non-related comorbidities
Abstract
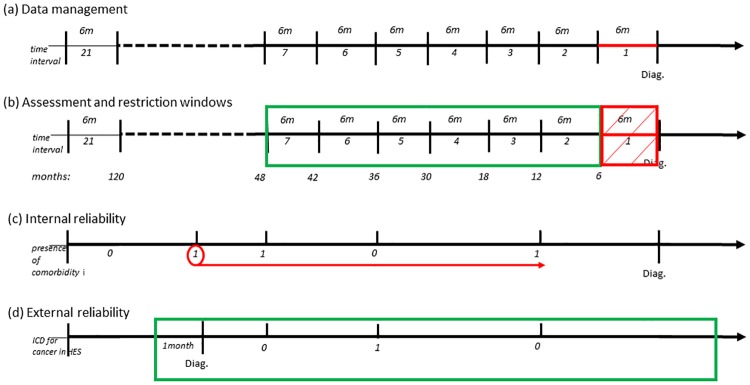
Background: Patients with comorbidities do not receive optimal treatment for their cancer, leading to lower cancer survival. Information on individual comorbidities is not straightforward to derive from population-based administrative health datasets. We described the development of a reproducible algorithm to extract the individual Charlson index comorbidities from such data. We illustrated the algorithm with 1,789 laryngeal cancer patients diagnosed in England in 2013. We aimed to clearly set out and advocate the time-related assumptions specified in the algorithm by providing empirical evidence for them.
Methods: Comorbidities were assessed from hospital records in the ten years preceding cancer diagnosis and internal reliability of the hospital records was checked. Data were right-truncated 6 or 12 months prior to cancer diagnosis to avoid inclusion of potentially cancer-related comorbidities. We tested for collider bias using Cox regression.
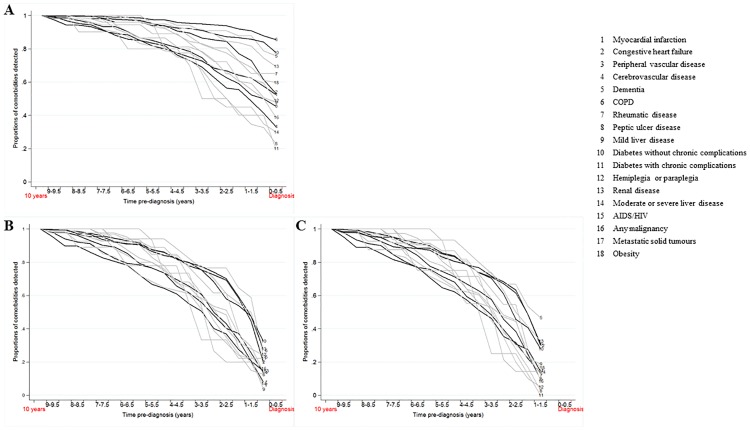
Results: Our administrative data showed weak to moderate internal reliability to identify comorbidities (ICC ranging between 0.1 and 0.6) but a notably high external validity (86.3%). We showed a reverse protective effect of non-cancer related Chronic Obstructive Pulmonary Disease (COPD) when the effect is split into cancer and non-cancer related COPD (Age-adjusted HR: 0.95, 95% CI:0.7-1.28 for non-cancer related comorbidities). Furthermore, we showed that a window of 6 years before diagnosis is an optimal period for the assessment of comorbidities.
Conclusion: To formulate a robust approach for assessing common comorbidities, it is important that assumptions made are explicitly stated and empirically proven. We provide a transparent and consistent approach useful to researchers looking to assess comorbidities for cancer patients using administrative health data.
Conflict of interest statement
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Tailored or adapted interventions for adults with chronic obstructive pulmonary disease and at least one other long-term condition: a mixed methods review.Cochrane Database Syst Rev. 2021 Jul 26;7(7):CD013384. doi: 10.1002/14651858.CD013384.pub2. Cochrane Database Syst Rev. 2021. PMID: 34309831 Free PMC article.
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Association of pre-existing comorbidities with mortality and disease severity among 167,500 individuals with COVID-19 in Canada: A population-based cohort study.PLoS One. 2021 Oct 5;16(10):e0258154. doi: 10.1371/journal.pone.0258154. eCollection 2021. PLoS One. 2021. PMID: 34610047 Free PMC article.
-
Validity of information on comorbidity derived rom ICD-9-CCM administrative data.Med Care. 2002 Aug;40(8):675-85. doi: 10.1097/00005650-200208000-00007. Med Care. 2002. PMID: 12187181
Cited by
-
Comparison of model-building strategies for excess hazard regression models in the context of cancer epidemiology.BMC Med Res Methodol. 2019 Nov 20;19(1):210. doi: 10.1186/s12874-019-0830-9. BMC Med Res Methodol. 2019. PMID: 31747928 Free PMC article.
-
Does previous asbestos exposure increase the risk of a post coronary artery bypass graft (CABG) pleural effusion - a routine data study?BMC Pulm Med. 2023 Aug 21;23(1):307. doi: 10.1186/s12890-023-02555-9. BMC Pulm Med. 2023. PMID: 37605147 Free PMC article.
-
Association between multimorbidity and socioeconomic deprivation on short-term mortality among patients with diffuse large B-cell or follicular lymphoma in England: a nationwide cohort study.BMJ Open. 2021 Nov 30;11(11):e049087. doi: 10.1136/bmjopen-2021-049087. BMJ Open. 2021. PMID: 34848510 Free PMC article.
-
Data-Adaptive Estimation for Double-Robust Methods in Population-Based Cancer Epidemiology: Risk Differences for Lung Cancer Mortality by Emergency Presentation.Am J Epidemiol. 2018 Apr 1;187(4):871-878. doi: 10.1093/aje/kwx317. Am J Epidemiol. 2018. PMID: 29020131 Free PMC article.
-
Health impact of monoclonal gammopathy of undetermined significance (MGUS) and monoclonal B-cell lymphocytosis (MBL): findings from a UK population-based cohort.BMJ Open. 2021 Feb 22;11(2):e041296. doi: 10.1136/bmjopen-2020-041296. BMJ Open. 2021. PMID: 33619185 Free PMC article.
References
-
- Glymour MM, Mayeda ER, Selby V. Selection bias in clinical epidemiology: causal thinking to guide patient-centered research. Epidemiology. 2016. - PubMed
-
- Fleming ST, Pursley HG, Newman B, Pavlov D, Chen K. Comorbidity as a Predictor of Stage of Illness for Patients With Breast Cancer. Medical care. 2005;43(2):132–40. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
