

Cognitive change trajectories in virally suppressed HIV-infected individuals indicate high prevalence of disease activity
- PMID: 28264037
- PMCID: PMC5338778
- DOI: 10.1371/journal.pone.0171887
Cognitive change trajectories in virally suppressed HIV-infected individuals indicate high prevalence of disease activity
Abstract
Background: The longitudinal rate and profile of cognitive decline in persons with stable, treated, and virally suppressed HIV infection is not established. To address this question, the current study quantifies the rate of cognitive decline in a cohort of virally suppressed HIV+ persons using clinically relevant definitions of decline, and determine cognitive trajectories taking into account historical and baseline HAND status.
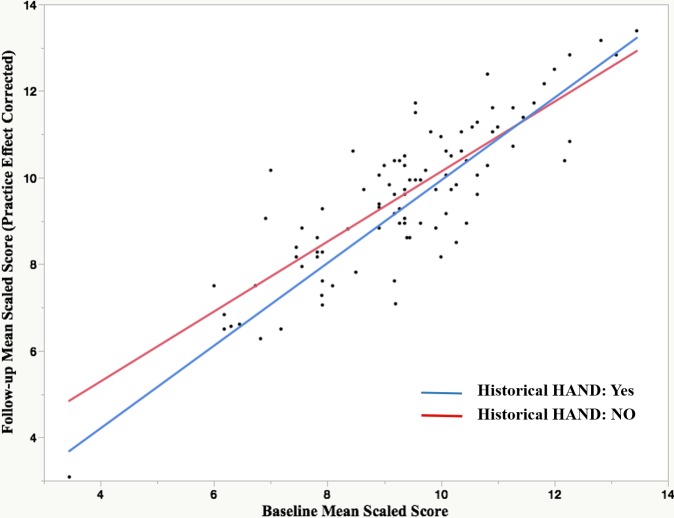
Methods: Ninety-six HIV+ (clinically stable and virally undetectable) and 44 demographically comparable HIV- participants underwent standard neuropsychological testing at baseline and 18-months follow-up. We described clinically relevant cognitive trajectories based on standard definitions of historical and baseline HAND status and cognitive decline. Historical, moderate to severe HAND was formally diagnosed at the start of the cART era in 15/96 participants based on clinical neurological and neuropsychological assessment. The same standard of care has been applied to all participants at St. Vincent's Hospital Infectious Disease Department for the duration of their HIV infection (median of 20 years).
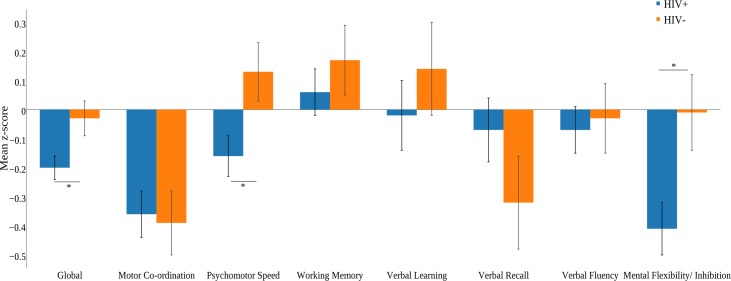
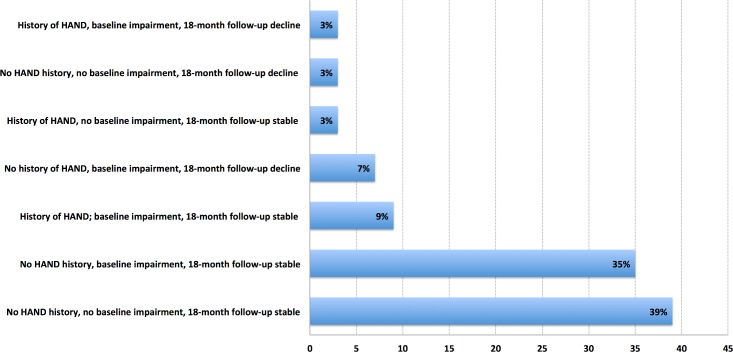
Results: Relative to HIV- controls (4.5%), 14% of HIV+ participants declined (p = .11), they also scored significantly lower on the global change score (p = .03), processing speed (p = .02), and mental flexibility/inhibition (p = .02) domains. Having HAND at baseline significantly predicted cognitive decline at follow up (p = .005). We determined seven clinically relevant cognitive trajectories taking into account whether participant has a history of HAND prior to study entry (yes/no); their results on the baseline assessment (baseline impairment: yes/no) and their results on the 18-month follow up (decline or stable) which in order of prevalence were: 1) No HAND history, no baseline impairment, 18-month follow-up stable (39%), 2) No HAND history, baseline impairment, 18-month follow-up stable (35%), 3) History of HAND; baseline impairment, 18-month follow-up stable (9%) 4) No history of HAND, baseline impairment, 18-month follow-up decline (7%), 5) History of HAND, no baseline impairment, 18-month follow-up stable (3%), 6) No HAND history, no baseline impairment, 18-month follow-up decline (3%) 7) History of HAND, baseline impairment, 18-month follow-up decline (3%). There was no relationship between cognitive decline (taking into account historical and baseline HAND) and traditional HIV disease biomarkers.
Conclusions: Despite long-term viral suppression, we found mostly subclinical levels of decline in psychomotor speed and executive functioning (mental flexibility and cognitive inhibition); well-established markers of HAND progression. Moreover, 57% of our cohort is undergoing slow evolution of their disease, challenging the notion of prevalent neurocognitive stability in virally suppressed HIV infection.
Conflict of interest statement
Figures
Similar articles
-
Meaningful cognitive decline is uncommon in virally suppressed HIV, but sustained impairment, subtle decline and abnormal cognitive aging are not.EClinicalMedicine. 2022 Dec 26;56:101792. doi: 10.1016/j.eclinm.2022.101792. eCollection 2023 Feb. EClinicalMedicine. 2022. PMID: 36618901 Free PMC article.
-
Pre-frailty predicts cognitive decline at 2-year follow-up in persons living with HIV.J Neurovirol. 2020 Apr;26(2):168-180. doi: 10.1007/s13365-019-00814-2. Epub 2019 Dec 19. J Neurovirol. 2020. PMID: 31858484 Free PMC article.
-
Cognitive Decline in Relation to Psychological Wellbeing and HIV Disease- and Treatment Characteristics in HIV-Infected Patients on cART: A One-Year Follow-Up Study.AIDS Behav. 2017 Jun;21(6):1728-1734. doi: 10.1007/s10461-016-1583-7. AIDS Behav. 2017. PMID: 27752871 Free PMC article.
-
HIV, Depression, and Cognitive Impairment in the Era of Effective Antiretroviral Therapy.Curr HIV/AIDS Rep. 2019 Feb;16(1):82-95. doi: 10.1007/s11904-019-00421-0. Curr HIV/AIDS Rep. 2019. PMID: 30661180 Free PMC article. Review.
-
HIV-Associated Neurocognitive Disorders: A Global Perspective.J Int Neuropsychol Soc. 2017 Oct;23(9-10):860-869. doi: 10.1017/S1355617717001102. J Int Neuropsychol Soc. 2017. PMID: 29198283 Free PMC article. Review.
Cited by
-
HIV-1 mRNA Knockdown with CRISPR/Cas9 Enhances Neurocognitive Function.Res Sq [Preprint]. 2023 Oct 16:rs.3.rs-3266933. doi: 10.21203/rs.3.rs-3266933/v1. Res Sq. 2023. Update in: J Neurovirol. 2024 Feb;30(1):71-85. doi: 10.1007/s13365-024-01193-z. PMID: 37886577 Free PMC article. Updated. Preprint.
-
Covertly active and progressing neurochemical abnormalities in suppressed HIV infection.Neurol Neuroimmunol Neuroinflamm. 2018 Jan 3;5(1):e430. doi: 10.1212/NXI.0000000000000430. eCollection 2018 Jan. Neurol Neuroimmunol Neuroinflamm. 2018. PMID: 29312999 Free PMC article.
-
Generating fair, reliable, and accurate neuropsychological test norms for people with HIV in a low- or middle-income country.J Neurovirol. 2025 Feb;31(1):41-55. doi: 10.1007/s13365-024-01235-6. Epub 2024 Dec 30. J Neurovirol. 2025. PMID: 39738926 Free PMC article.
-
Neuroinflammatory transcriptional programs induced in rhesus pre-frontal cortex white matter during acute SHIV infection.J Neuroinflammation. 2022 Oct 6;19(1):250. doi: 10.1186/s12974-022-02610-y. J Neuroinflammation. 2022. PMID: 36203187 Free PMC article.
-
Non-Human Primate Models of HIV Brain Infection and Cognitive Disorders.Viruses. 2022 Sep 9;14(9):1997. doi: 10.3390/v14091997. Viruses. 2022. PMID: 36146803 Free PMC article. Review.
References
-
- The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia. Annual Surveillance Reports 2015 [Internet]. 2015. Available: http://www.kirby.unsw.edu.au/surveillance/Annual-Surveillance-Reports
-
- Reger M, Welsh R, Razani J, Martin DJ, Boone KB. A meta-analysis of the neuropsychological sequelae of HIV infection. J Int Neuropsychol Soc. 2002;8: 410–424. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
